预约演示
更新于:2025-08-27

Innovent Biologics, Inc.
更新于:2025-08-27
概览
标签
肿瘤
内分泌与代谢疾病
消化系统疾病
ADC
单克隆抗体
小分子化药
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

NCT07120425
A Single Ascending Dose Study to Evaluate the Safety, Tolerability and Pharmacokinetics of IBI3032 in Healthy Participants
NCT07124793
Phase II Study to Evaluate the Efficacy and Safety of IBI363 in Combination With IBI305 in Participants With Advanced Solid Tumors
NCT07122687
A Phase II Study Evaluating the Efficacy and Safety of IBI363 Combined With Chemotherapy or Pembrolizumab Combined With Chemotherapy as Neoadjuvant Therapy in Resectable Stage IB-III Non-Squamous Non-Small Cell Lung Cancer
100 项与 信达生物制药 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-05-01Med
IBI310 plus sintilimab vs. placebo plus sintilimab in recurrent/metastatic cervical cancer: A double-blind, randomized controlled trial
Article
作者: Tang, Yaling ; Zhang, Guonan ; Huang, Yi ; Ma, Xinyan ; Li, Huayi ; Zhao, Weidong ; Qian, Jianhua ; Xu, Qin ; Zhang, Jieqing ; Zheng, Hong ; Wang, Danbo ; Zhou, Hui ; Gao, Qinglei ; Tang, Ying ; Peng, Zikun ; Qiu, Hui ; Ji, Jianghai ; Yin, Kang ; Liu, Jihong ; Cai, Chujun ; An, Ruifang ; Shen, Yiyang ; Wang, Li ; Zhang, Hongfei ; Wang, Shuyan ; Xie, Han ; Wang, Xia ; Li, Guiling ; Chang, Baoping ; Yuan, Jianlin ; Ma, Cailing ; Sun, Li ; He, Aiqin ; Jiao, Xiaofei ; Zhu, Lijing ; Xu, Yu ; Wang, Ya ; Zhu, Jianqing ; Lou, Ge ; Wang, Jing ; Xia, Bairong ; Ma, Ding ; Duan, Wei ; Lu, Liqin ; Wang, Ke ; Li, Li ; Zhu, Hong ; Cheng, Yan ; Yu, Guohua ; Huang, Jianli ; Chen, Youguo ; Huang, Bowen ; Zhang, Youzhong
BACKGROUND:
It remains unclear whether adding CTLA-4 blockade to PD-1/PD-L1 blockade improves clinical outcomes in cervical cancer (CC).
METHODS:
In this randomized, double-blind, placebo-controlled, phase 2 study (ClinicalTrials.gov: NCT04590599), patients with recurrent/metastatic CC (R/M CC) who experienced disease progression after or during platinum-based chemotherapy were enrolled from 37 centers across China and randomly assigned (1:1), stratified by PD-L1 expression and prior treatment lines, to receive either IBI310 plus sintilimab or placebo plus sintilimab intravenously every 3 weeks for 12 weeks, followed by sintilimab alone. The primary endpoint was the objective response rate (ORR). Pivotal secondary endpoints included progression-free survival (PFS), overall survival (OS), and safety.
FINDINGS:
205 patients were randomized to receive IBI310-sintilimab (n = 103) or placebo-sintilimab (n = 102). The ORR difference between the IBI310-sintilimab arm (32.3%, 95% confidence interval [CI]: 23.3%-42.5%) and the placebo-sintilimab arm (23.5%, 95% CI: 15.5%-33.1%) was not significant (p = 0.17). IBI310-sintilimab and placebo-sintilimab exhibited median PFS values of 3.6 (95% CI: 2.7-6.3) and 4.2 months (95% CI: 2.8-6.2), respectively (hazard ratio [HR] = 0.91, 95% CI: 0.65-1.27; p = 0.58). The median OSs were 13.9 months (95% CI: 11.5-25.6) in the IBI310-sintilimab arm and 17.2 months (95% CI: 13.7-25.9) in the placebo-sintilimab arm (HR = 1.12, 95% CI: 0.79-1.58; p = 0.54). Adding IBI310 to sintilimab increased the incidence of grade ≥3 treatment-related adverse events (55% versus 19%).
CONCLUSIONS:
Compared to single-agent PD-1/PD-L1 blockade, dual blockade of CTLA-4 and PD-1/PD-L1 did not significantly improve clinical outcomes in R/M CC.
FUNDING:
This work was funded by Innovent Biologics (Suzhou).
2025-02-01Ophthalmology Retina
Efficacy and Safety of Efdamrofusp Alfa versus Aflibercept in Participants with Neovascular Age-Related Macular Degeneration
Article
作者: Li, Jinying ; Wen, Ying ; Lu, Shujie ; Yu, Songping ; He, Tao ; Li, Haoyu ; Wang, Xian ; Xu, Yihua ; Wei, Wenbin ; Dai, Hong ; Tong, Jianping ; Zhang, Wenfang ; Jia, Huixun ; Wang, Wei ; Wu, Miaoqin ; Zhang, Jinglin ; Zheng, Qinxiang ; Pei, Cheng ; Li, Mingxin ; Liu, Qinghuai ; Deng, Junjie ; Mao, Junfeng ; Cui, Ling ; Ye, Jian ; Gong, Yuanyuan ; Hao, Jilong ; Guan, Huaijin ; Liu, Xiaoling ; Tao, Liming ; Yan, Ming ; Bi, Yanlong ; Qian, Lei ; Shu, Xiangwen ; Ding, Lin ; Sun, Xiaodong ; Peng, Hui ; Fan, Ke ; Li, Chaopeng ; Song, Yanping ; Xu, Xiangzhong ; Wu, Zhifeng ; Zhao, MingWei ; Sun, Junran ; Wang, Hong ; Zhu, Dan ; Liu, Wei ; Wang, Feng ; Lu, Peirong
PURPOSE:
To evaluate efficacy and safety of efdamrofusp alfa compared with aflibercept in neovascular age-related macular degeneration (nAMD).
DESIGN:
Randomized, double-masked, multicenter, active-controlled, noninferiority phase II study.
PARTICIPANTS:
A total of 231 treatment-naive and previously treated participants with active choroidal neovascularization secondary to nAMD were enrolled.
METHODS:
Eligible participants were randomized (1:1:1) to 2 mg efdamrofusp alfa, 4 mg efdamrofusp alfa, or 2 mg aflibercept groups. Participants in all groups received 3 initial monthly loading doses, followed by treatment every 8 weeks, with assessment every 4 weeks up to week 52.
MAIN OUTCOME MEASURES:
The primary end point was the mean best-corrected visual acuity (BCVA) change from baseline to week 36. The prespecified noninferiority margin was set as -5 letters (80% confidence interval [CI]).
RESULTS:
Each treatment group included 77 participants. The mean BCVA changes from baseline to week 36 for 2 mg efdamrofusp alfa, 4 mg efdamrofusp alfa and aflibercept groups were +10.6, +11.4, and +12.0 letters, respectively; least squares mean difference were -1.4 (80% CI: -3.5 to 0.7) between 2 mg efdamrofusp alfa and aflibercept, and -0.6 (80% CI: -2.7 to 1.6) between 4 mg efdamrofusp alfa and aflibercept. Mean central retinal thickness changes were consistent across groups. Adverse event rate was comparable among the groups.
CONCLUSIONS:
Efdamrofusp alfa demonstrated noninferiority to aflibercept in BCVA improvement, accompanied by a similar safety profile.
FINANCIAL DISCLOSURE(S):
The author(s) have no proprietary or commercial interest in any materials discussed in this article.
2025-02-01Med
A tumor cornification and immune-infiltration-based scheme for anti-PD-1 plus chemotherapy response in advanced squamous cell lung carcinoma
Article
作者: Sun, Jiya ; Wang, Lei ; Hu, Congli ; Cheng, Lei ; Wu, Fengying ; Li, Xuefei ; Wu, Lin ; Zhou, Caicun ; Jiang, Minlin ; Fan, Yun ; Gao, Guanghui ; Liu, Lianke ; Wu, Chunyan ; Zhou, Hui ; Li, Fei ; Peng, Bo ; Wang, Zhehai
BACKGROUND:
Anti-PD-1 immunotherapy plus chemotherapy (combo) exhibits significantly prolonged survival for squamous cell lung cancer (LUSC). An exploration of predictive biomarkers is still needed.
METHODS:
High-throughput RNA sequencing (RNA-seq) of 349 LUSC samples from the randomized, multi-center, phase 3 trial ORIENT-12 (ClinicalTrials.gov: NCT03629925) was conducted for biomarker discovery, followed by flow cytometry and multiplex immunohistochemistry (mIHC) in additional clinical cohorts, and in vitro experiments were performed for verification.
RESULTS:
A high abundance of activated CD8+ T and CD56bright natural killer (NK) cells benefited patients' outcomes (progression-free survival [PFS]; overall survival [OS]) with combo treatment. Tumor cornification level remarkably affected the infiltration of the two crucial immune cells. Thus, a novel scheme of LUSC immune infiltration and cornification characterization-based classification (LICC) was established for combo efficacy prediction. Patients who received combo treatment achieved significant PFS improvements in LICC1 (hazard ratio [HR] = 0.43, 95% confidence interval [CI]: 0.25-0.75, p = 0.0029) and LICC2 (HR = 0.32, 95% CI: 0.17-0.58, p = 0.0002) subtypes but not in the LICC3 subtype (HR = 0.86, 95% CI: 0.60-1.23, p = 0.4053). Via single-cell RNA-seq analysis, the tumor cornification signal was mainly mapped to SPRR3+ tumor cells, whose relationships with activated CD8+ T or CD56bright NK cells were verified using flow cytometry and mIHC. Our data suggest that SPRR3+ tumor cells might evade immune surveillance via the CD24-SIGLEC10 (M2 macrophage) axis to maintain a suppressive tumor microenvironment.
CONCLUSIONS:
Tumor cornification greatly impacts immune infiltration, and the LICC scheme may guide clinical medication of anti-PD-1+chemo treatment in patients with LUSC.
FUNDING:
The study was funded by the National Key R&D Program of China, the National Natural Science Foundation of China, Shanghia Multidisplinary Cooperation Building Project for Diagnosis and Treatment of Major Disease, and Innovent Biologics, Inc.
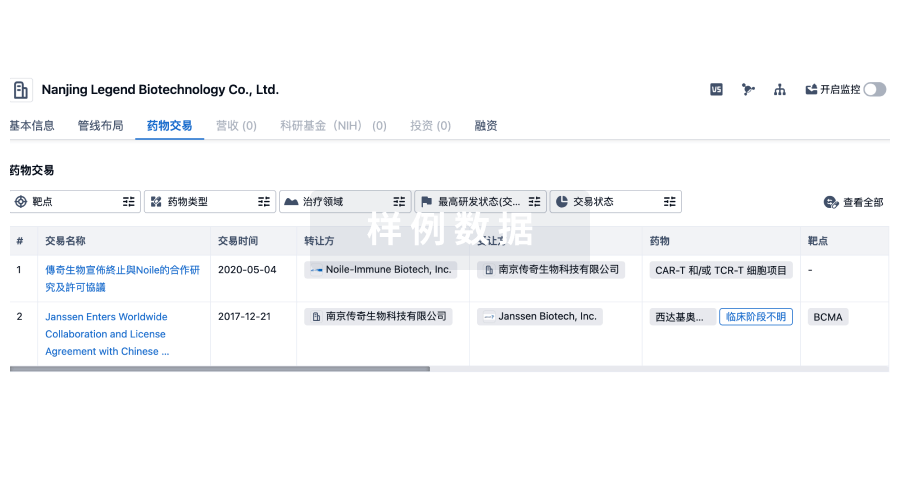
100 项与 信达生物制药 相关的药物交易
登录后查看更多信息
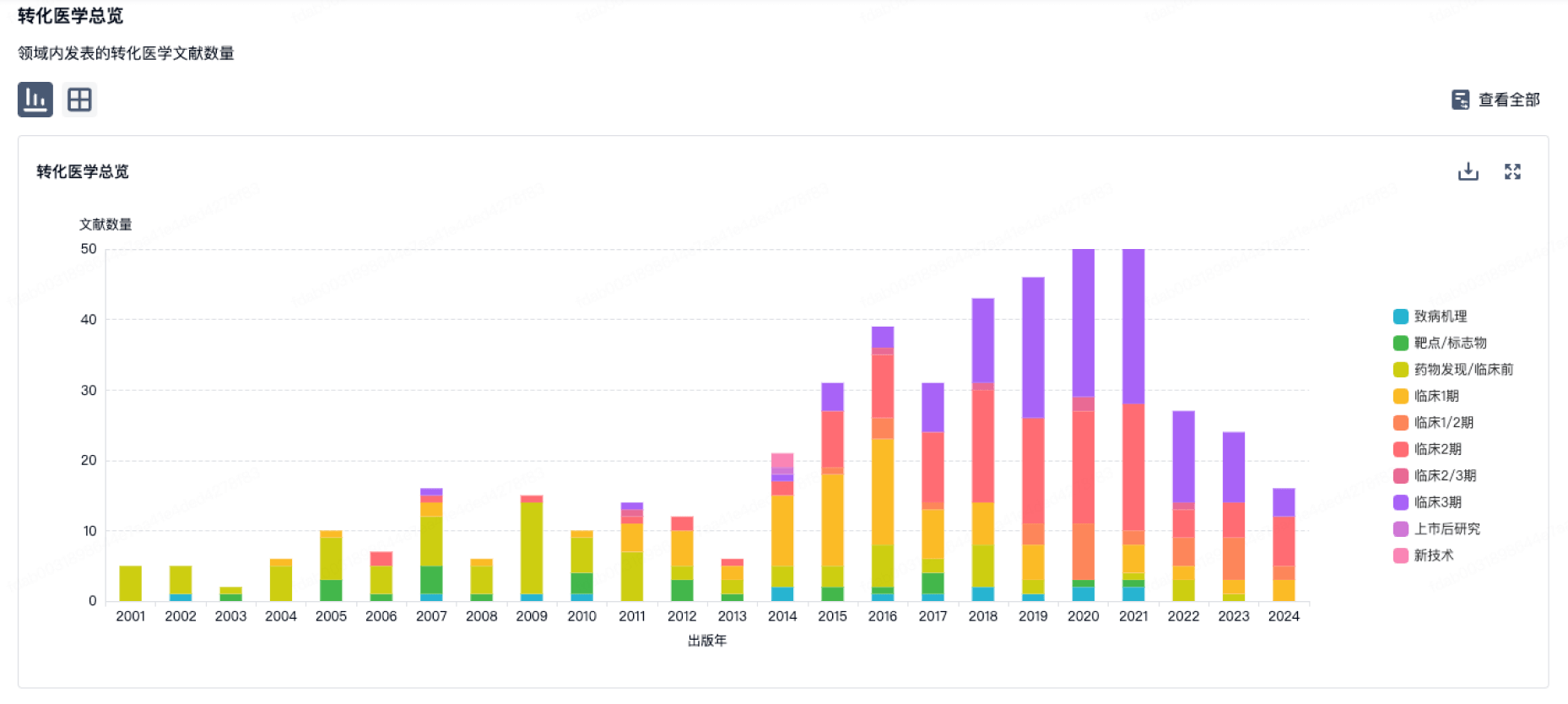
100 项与 信达生物制药 相关的转化医学
登录后查看更多信息
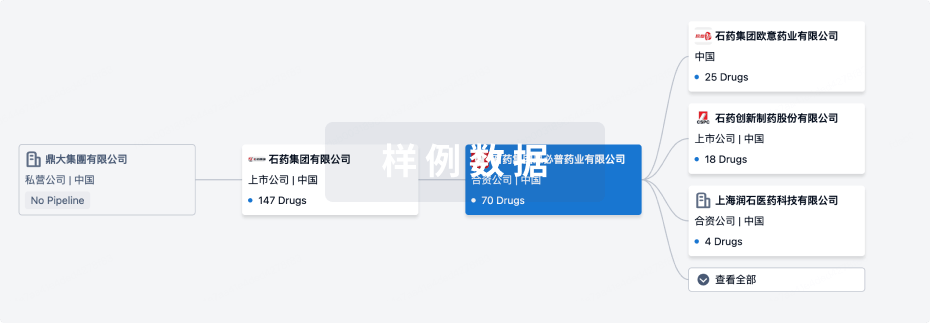
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年09月02日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
10
25
临床前
临床申请
4
5
临床申请批准
临床1期
20
9
临床2期
临床3期
4
4
申请上市
批准上市
12
29
其他
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
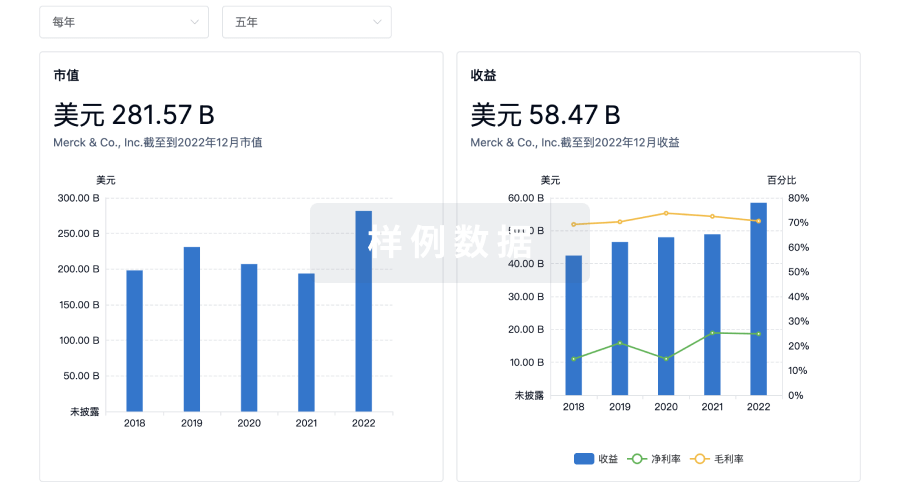
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用