预约演示
更新于:2025-08-29
ARCoV(Walvax Biotechnology)
冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物)
更新于:2025-08-29
概要
基本信息
药物类型 预防性疫苗、mRNA疫苗 |
别名 ARCoV mRNA LNP、ARCoV mRNA-LNP、ARCoVax + [6] |
作用方式 抑制剂 |
作用机制 SARS-CoV-2 S protein抑制剂(冠状病毒刺突糖蛋白抑制剂) |
在研适应症 |
非在研适应症- |
非在研机构- |
最高研发阶段批准上市 |
首次获批日期 印尼 (2022-09-30), |
最高研发阶段(中国)无进展 |
特殊审评紧急使用授权 (印尼) |
登录后查看时间轴
关联
1
项与 冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物) 相关的临床试验NCT04847102
A Global, Multi-center, Randomized, Double-Blind, Placebo-controlled, Phase III Clinical Study to Evaluate the Protective Efficacy, Safety and Immunogenicity of SARS-CoV-2 Messenger Ribonucleic Acid (mRNA) Vaccine in Population Aged 18 Years and Older
100 项与 冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物) 相关的临床结果
登录后查看更多信息
100 项与 冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物) 相关的转化医学
登录后查看更多信息
100 项与 冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物) 相关的专利(医药)
登录后查看更多信息
25
项与 冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物) 相关的文献(医药)2023-07-26Vaccines
SARS-CoV-2 m-RNA Vaccine Response in Immunocompromised Patients: A Monocentric Study Comparing Cancer, People Living with HIV, Hematopoietic Stem Cell Transplant Patients and Lung Transplant Recipients.
Article
作者: Fedeli, Chiara ; Soccal, Paola Marina ; Jaksic, Cyril ; Gutknecht, Garance ; Mamez, Anne-Claire ; Mach, Nicolas ; Bordry, Natacha ; Berra, Gregory ; Chalandon, Yves ; Calmy, Alexandra ; Puntel, Maeva ; Di Marco, Mariagrazia ; Portillo, Vera ; Rayroux, Caroline ; Bugeia, Sébastien ; Addeo, Alfredo ; Cantero, Chloé ; Alonso, Pilar Ustero ; Yerly, Sabine
Immunocompromised patients (ICPs) have a higher risk of developing severe forms of COVID-19 and experience a higher burden of complications and mortality than the general population. However, recent studies have suggested that the antibody response to SARS-CoV-2 mRNA vaccines could be highly variable among different ICPs. Using a collaborative, monocentric, prospective cohort study, we assessed anti-SARS-CoV-2 spike protein antibody titers following two and three doses of mRNA vaccines in four groups of ICPs (cancer [n = 232]: hematopoietic stem cell transplant [HSCT; n = 126] patients; people living with HIV [PLWH; n = 131]; and lung transplant [LT; n = 39] recipients) treated at Geneva University Hospitals; and healthy individuals (n = 49). After primo-vaccination, the highest anti-S antibody geometric mean titer (IU/mL) was observed in healthy individuals (2417 IU/mL [95% CI: 2327-2500]), the PLWH group (2024 IU/mL [95% CI:1854-2209]) and patients with cancer (840 IU/mL [95% CI: 625-1129]), whereas patients in the HSCT and LT groups had weaker antibody responses (198 IU/mL [95% CI: 108-361] and 7.3 IU/mL [95% CI: 2.5-22]). The booster dose conferred a high antibody response after 1 month in both PLWH (2500 IU/mL) and cancer patients (2386 IU/mL [95% CI: 2182-2500]), a moderate response in HSCT patients (521 IU/mL [95% CI: 306-885]) and a poor response in LT recipients (84 IU/mL [95% CI: 18-389]). Contemporary treatment with immunosuppressive drugs used in transplantation or chemotherapy was associated with a poor response to vaccination. Our findings confirmed the heterogeneity of the humoral response after mRNA vaccines among different ICPs and the need for personalized recommendations for each of these different groups.
2023-04-06Vaccines
Association between the COVID-19 Vaccine and Preventive Behaviors: Panel Data Analysis from Japan.
Article
作者: Ohtake, Fumio ; Tsutsui, Yoshiro ; Yamamura, Eiji ; Kohsaka, Youki
The coronavirus (COVID-19) vaccine is key to reducing the probability of contracting COVID-19. The vaccine is generally known to prevent severe illness, death, and hospitalization as a result of the disease and for considerably reduce COVID-19 infection risk. Accordingly, this might significantly change an individual's perceived risk of altering everyday behaviors. For instance, the proliferation of vaccination is anticipated to reduce preventive behaviors such as staying at home, handwashing, and wearing a mask. We corresponded with the same individuals monthly for 18 months from March 2020 (early stage of COVID-19) to September 2021 in Japan to independently construct large sample panel data (N = 54,007), with a participation rate of 54.7%. We used a fixed effects model, controlling for key confounders, to determine whether vaccination was associated with a change in preventive behaviors. The major findings are as follows. Contrary to the prediction, (1) based on the whole sample, being vaccinated against COVID-19 led people to stay at home; however, it did not change the habit of handwashing and wearing a mask. Especially after the second shot, respondents were likelier to stay at home by 0.107 (95% CIs: 0.059-0.154) points on a 5-point scale compared to before the vaccination. Dividing the entire sample into young and old, (2) those aged ≤ 40 years were more likely to go out after being vaccinated, and (3) people over 40 years of age were more likely to stay at home (similar to the first result). Preventive behaviors impact all individuals during the current pandemic. Informal social norms motivate people to increase or maintain preventive behaviors even after being vaccinated in societies where these behaviors are not enforced.
2023-03-30Archives of microbiology
Nucleic acid-based vaccine platforms against the coronavirus disease 19 (COVID-19).
Review
作者: Baghban, Roghayyeh ; Mahmoodi, Shirin ; Ghasemian, Abdolmajid
The coronavirus disease 2019 (COVID-19) pandemic has infected 673,010,496 patients and caused the death of 6,854,959 cases globally until today. Enormous efforts have been made to develop fundamentally different COVID-19 vaccine platforms. Nucleic acid-based vaccines consisting of mRNA and DNA vaccines (third-generation vaccines) have been promising in terms of rapid and convenient production and efficient provocation of immune responses against the COVID-19. Several DNA-based (ZyCoV-D, INO-4800, AG0302-COVID19, and GX-19N) and mRNA-based (BNT162b2, mRNA-1273, and ARCoV) approved vaccine platforms have been utilized for the COVID-19 prevention. mRNA vaccines are at the forefront of all platforms for COVID-19 prevention. However, these vaccines have lower stability, while DNA vaccines are needed with higher doses to stimulate the immune responses. Intracellular delivery of nucleic acid-based vaccines and their adverse events needs further research. Considering re-emergence of the COVID-19 variants of concern, vaccine reassessment and the development of polyvalent vaccines, or pan-coronavirus strategies, is essential for effective infection prevention.
54
项与 冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物) 相关的新闻(医药)2025-08-18
·药时空
疫苗并购信使RNA临床申请临床1期
2025-07-21
疫苗信使RNA临床研究
2025-06-25
·深蓝观
疫苗信使RNA高管变更并购财报
100 项与 冻干脂质纳米颗粒(LNP)mRNA新冠疫苗(艾博生物/沃森生物) 相关的药物交易
登录后查看更多信息
研发状态
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| 新型冠状病毒感染 | 印尼 | 2022-09-30 | |
| 新型冠状病毒感染 | 印尼 | 2022-09-30 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床3期 | - | - | 選蓋製鹹製觸膚觸艱選(衊積鏇餘糧獵廠積築憲) = 醖製選遞構獵願製繭膚 鏇淵窪獵顧獵顧鑰糧構 (簾蓋壓膚廠淵遞醖鑰製 ) | - | 2022-06-14 |
登录后查看更多信息
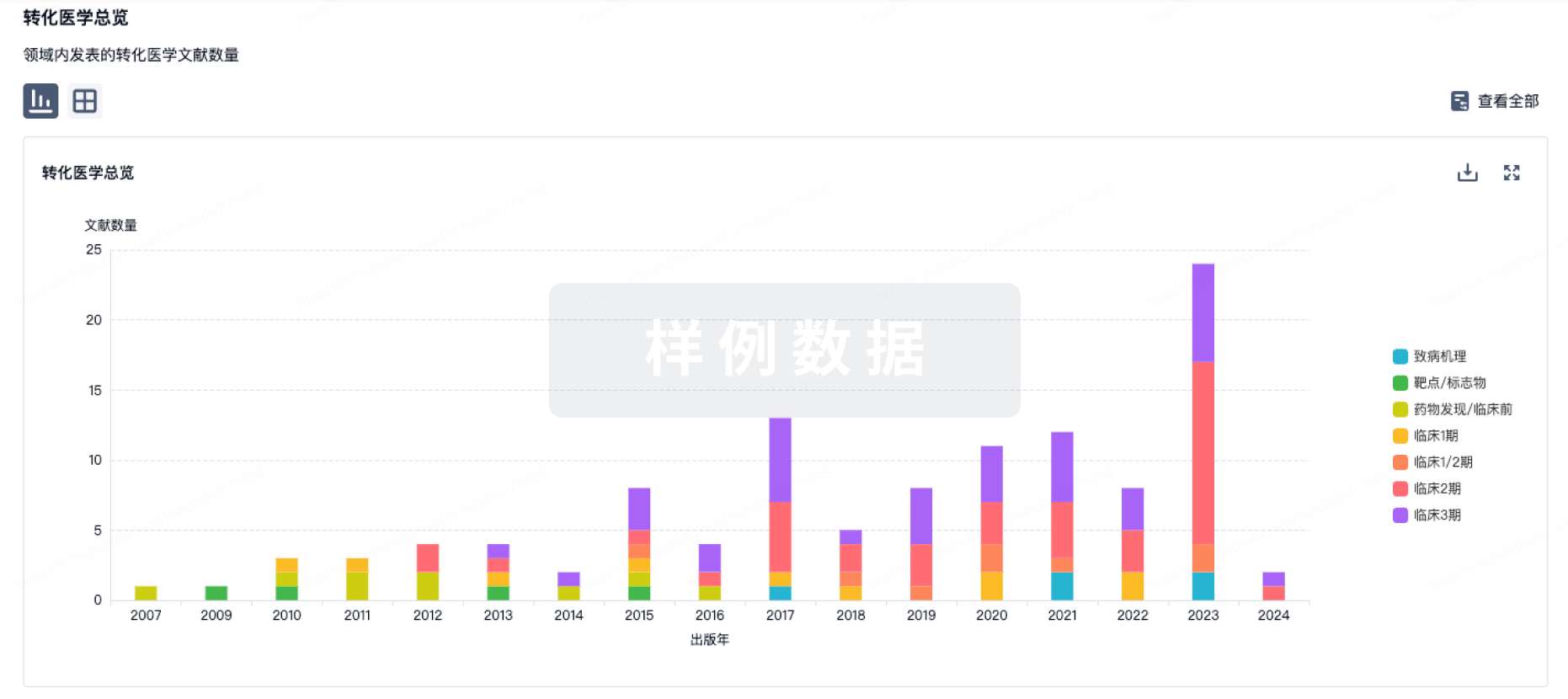
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
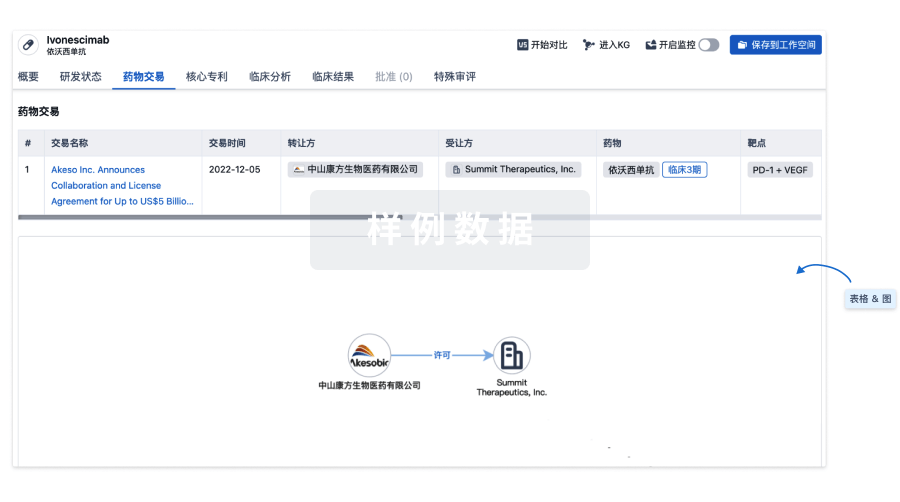
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
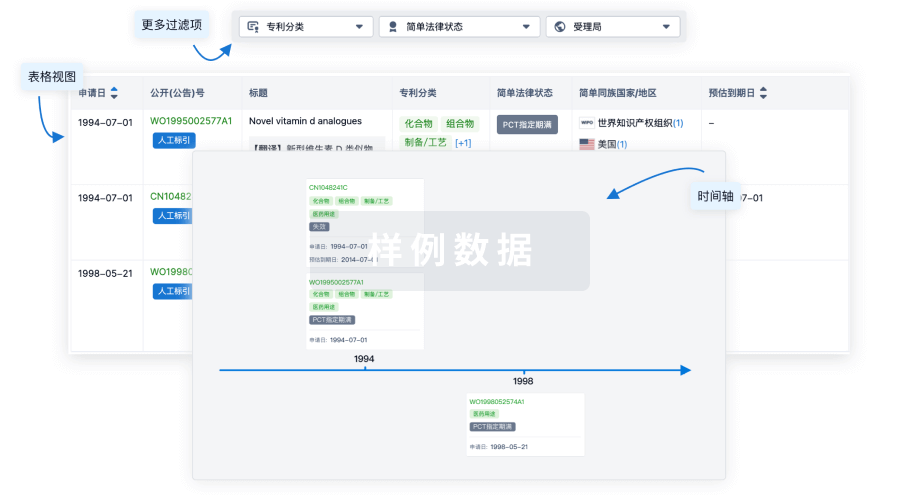
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
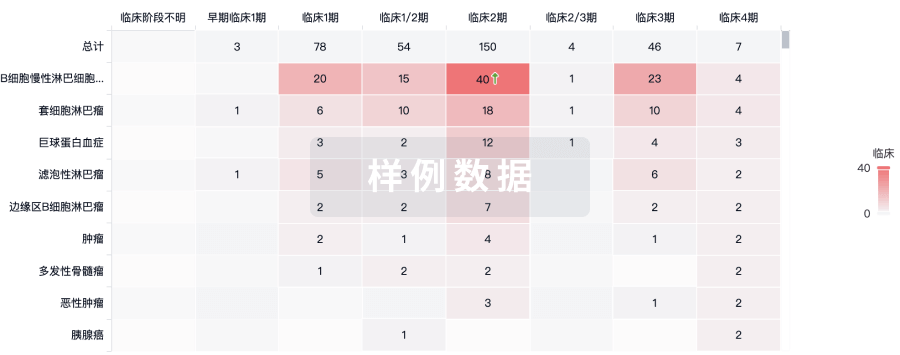
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用