预约演示
更新于:2025-05-07
Lp(a)
更新于:2025-05-07
基本信息
别名 lipoprotein(a)、LP、Lp(a) + [1] |
简介 Apo(a) is the main constituent of lipoprotein(a) (Lp(a)). It has serine proteinase activity and is able of autoproteolysis. Inhibits tissue-type plasminogen activator 1. Lp(a) may be a ligand for megalin/Gp 330. |
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |


靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
NCT06813911
A Randomized, Double-blind, Placebo-controlled, Multicenter Study to Evaluate the Efficacy, Safety, and Tolerability of Pelacarsen (TQJ230) With Background Inclisiran in Participants With Atherosclerotic Cardiovascular Disease (ASCVD), and Elevated LDL-C and Lp(a)

NCT06875973
A Rollover Extension Program (REP) to Evaluate the Long-term Safety and Tolerability of Open-Label Pelacarsen in Participants With Elevated Lp(a) and Established ASCVD
NCT06916078
A Phase 1, Multicenter, Sequential-Design, Single-Dose, Open-Label Study of Lepodisiran in Participants With Normal Hepatic Function and Participants With Mild, Moderate, or Severe Hepatic Impairment
100 项与 Lp(a) 相关的临床结果
登录后查看更多信息
100 项与 Lp(a) 相关的转化医学
登录后查看更多信息
登录后查看更多信息
2025-12-31Clinical and Experimental Hypertension
Relationship between lipoprotein B and the severity of coronary microvascular dysfunction
Article
作者: Yang, Lili ; Zhang, Jingjing ; Han, Jiangyan ; Jiang, Xiaojuan
2025-12-31The Journal of Maternal-Fetal & Neonatal Medicine
Relationship between ApoA-1, ApoB/ApoA-1 ratio, and preterm birth in patients with gestational diabetes mellitus in the third trimester
Article
作者: Yu, Juan ; Xiao, Min ; Chen, Ying-ying
2025-12-31Annals of Medicine
Persistent lipoprotein(a) exposure and its association with clinical outcomes after acute myocardial infarction: a longitudinal cohort study
Article
作者: Fang, Lijuan ; Liu, Naifeng ; Tang, Junnan ; Zhang, Jinying ; Wang, Zhenwei ; Shi, Qian
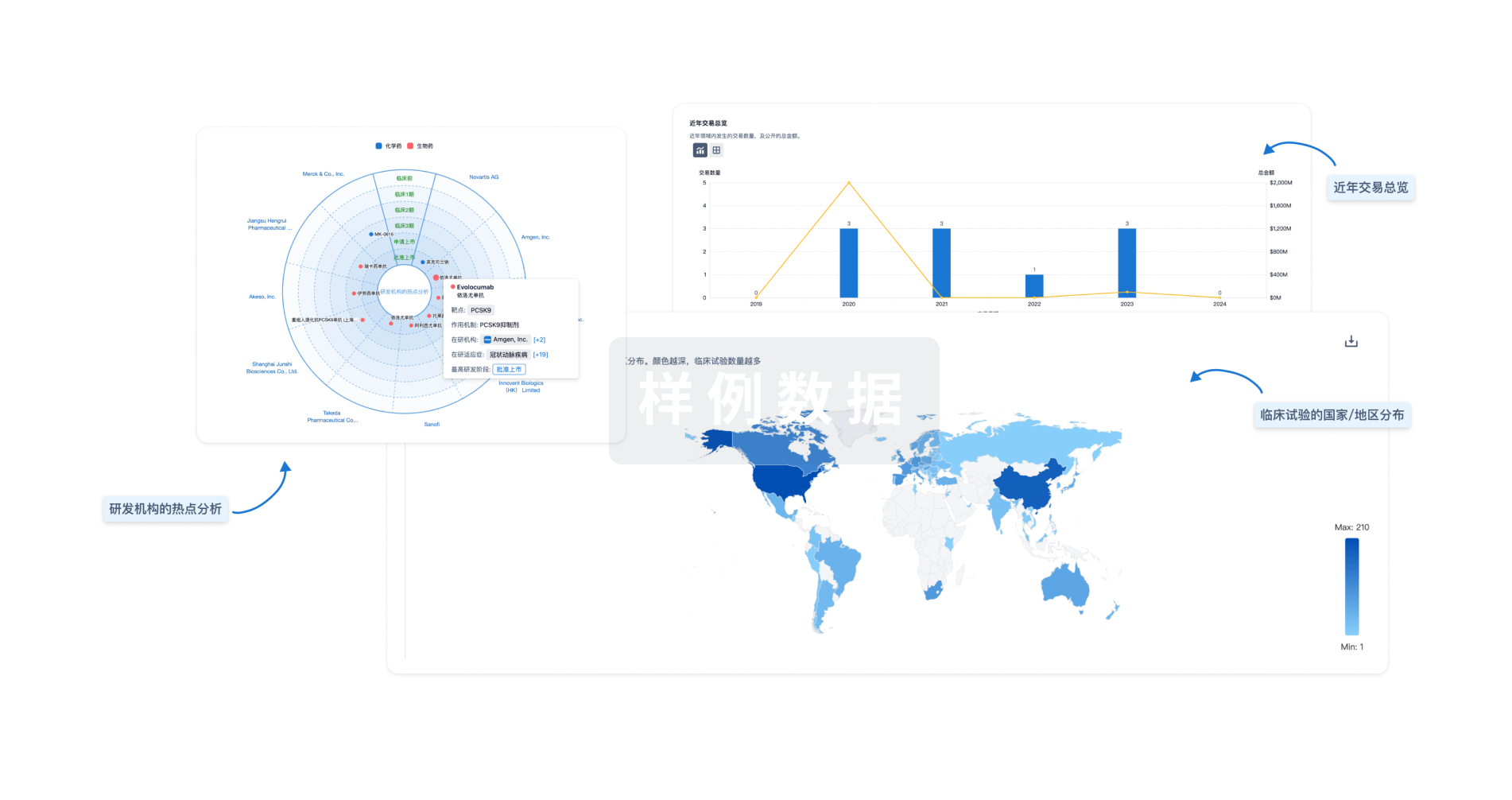
分析
对领域进行一次全面的分析。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用