预约演示
更新于:2025-05-07
RARγ
更新于:2025-05-07
基本信息
别名 NR1B3、Nuclear receptor subfamily 1 group B member 3、RAR-gamma + [5] |
简介 Receptor for retinoic acid. Retinoic acid receptors bind as heterodimers to their target response elements in response to their ligands, all-trans or 9-cis retinoic acid, and regulate gene expression in various biological processes. The RAR/RXR heterodimers bind to the retinoic acid response elements (RARE) composed of tandem 5'-AGGTCA-3' sites known as DR1-DR5. In the absence of ligand, acts mainly as an activator of gene expression due to weak binding to corepressors. Required for limb bud development. In concert with RARA or RARB, required for skeletal growth, matrix homeostasis and growth plate function (By similarity). |
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |


靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |


靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

NCT06908954
A Phase I, Open-label, Parallel-group Study to Evaluate the Single-dose Pharmacokinetics of Palovarotene in Male and Female Participants With Moderate and Severe Hepatic Impairment and Matched Participants With Normal Hepatic Function
CTRI/2024/08/072412
A prospective, multi center, open label phase IV clinical study to evaluate the safety and efficacy of Trifarotene or Aklief 50 microgram per gram cream in subjects with acne vulgaris over 12 weeks. - NIL
NCT06733402
A Multi-center, Double-blind, Randomized, Placebo Controlled, Parallel-group Study, Comparing Trifarotene Cream 0.005% (Taro Pharmaceuticals U.S.A, Inc.) to Aklief® Cream (US REFERENCE LISTED DRUG), Aklief Cream (REFERENCE PRODUCT) and Each Active Treatment to a Placebo Control in the Treatment of Acne Vulgaris.
100 项与 RARγ 相关的临床结果
登录后查看更多信息
100 项与 RARγ 相关的转化医学
登录后查看更多信息
登录后查看更多信息
2025-07-01Critical Reviews in Oncology/Hematology
Pharmacogenomics in pediatric oncology patients with solid tumors related to chemotherapy-induced toxicity: A systematic review
Review
作者: Uvdal, Hanna ; Hansson, Paula ; Blacker, Christopher ; Wadelius, Mia ; Green, Henrik ; Ljungman, Gustaf
2025-04-21Journal of Bone and Mineral Research
Retinoid-impregnated nanoparticles enable control of bone growth by site-specific modulation of endochondral ossification in mice
Article
作者: Suzuki, Akiko ; Alferiev, Ivan ; Tian, Hongying ; Matsuoka, Masatake ; Abzug, Joshua M ; Oichi, Takeshi ; Iwamoto, Masahiro ; Enomoto-Iwamoto, Motomi ; Otsuru, Satoru ; Pacifici, Maurizio ; Herzenberg, John E ; Tang, Ningfeng ; Usami, Yu ; Uchibe, Kenta ; Chorny, Michael
2025-04-01Cancer Genetics
Complex genetic structural aberrations revealed by optical genome mapping in a case of APL-like morphology
Article
作者: Karrs, Jeremiah X ; Steinmetz, Heather B ; Smuliac, Narcisa A ; Murad, Farzana ; Sathyanarayana, Shivaprasad H ; Sullivan, Matthew R ; Bickford, Michelle A ; Khan, Wahab A ; Bao, Jing ; Kaur, Prabhjot ; Tonseth, Kyle A
2024-12-01

临床结果临床研究
2024-09-06
临床申请临床2期临床1期申请上市临床结果
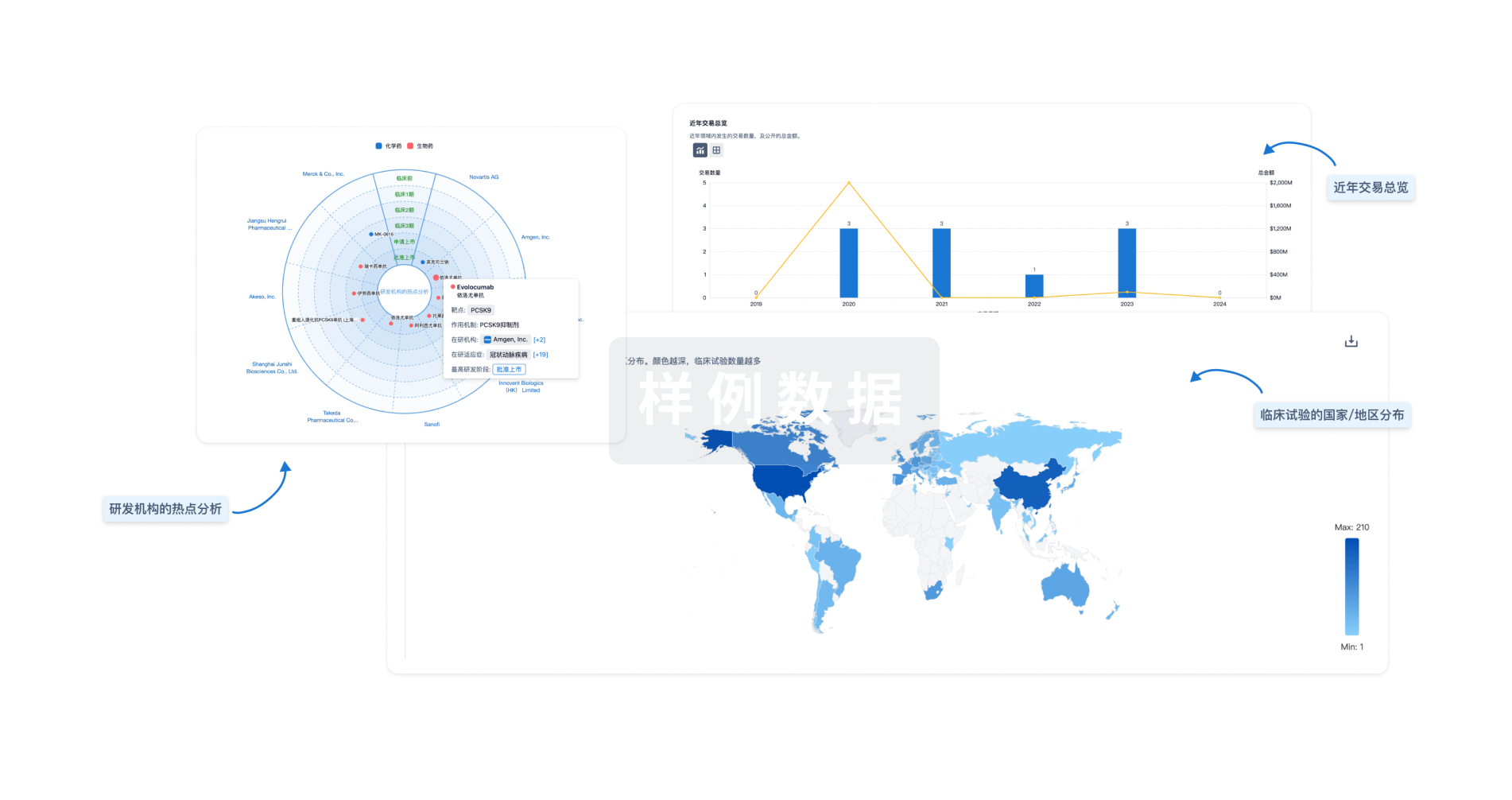
分析
对领域进行一次全面的分析。
登录
或
生物医药百科问答
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用