预约演示
更新于:2025-08-17
Shenzhen Kangtai Biological Products Co., Ltd.
更新于:2025-08-17
概览
标签
感染
呼吸系统疾病
其他疾病
预防性疫苗
联合疫苗
多价疫苗
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
CTR20251982
评价吸附无细胞百白破(组分)联合疫苗应用于健康婴幼儿的安全性和免疫原性的随机、盲法、平行阳性对照Ⅲ期临床试验
CTR20251014
评价口服五价重配轮状病毒减毒活疫苗(Vero细胞)在中国婴幼儿中的有效性、安全性和免疫原性的多中心、随机、双盲、安慰剂对照的Ⅲ期临床试验
CTR20251162
评价四价肠道病毒灭活疫苗(Vero细胞)在6月龄及以上健康人群中免疫的安全性和初步免疫原性的部分随机、盲态、阳性对照Ⅰ期临床试验。
100 项与 深圳康泰生物制品股份有限公司 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-12-31Expert Review of Vaccines
Immunogenicity and safety of a live attenuated varicella vaccine in healthy subjects aged between 13 to 55 years: a double-blind, randomized, active-controlled phase III clinical trial in China
Article
作者: Li, Jingxin ; Zhang, Yang ; Sun, Jinfang ; Zhang, Hao ; Zhu, Fengcai ; Pan, Hongxing ; Li, Guifan ; Wang, Shiyuan ; Shi, Jinhui ; Chang, Xianyun
BACKGROUND:
Adolescents and adults who contract chickenpox are at a higher risk of severe complications. Vaccination with the varicella vaccine (VarV) effectively prevents chickenpox.
RESEARCH DESIGN AND METHODS:
In this phase III, single-center, randomized, double-blind, active-controlled trial, 1,200 healthy participants were randomly assigned in a 1:1 ratio to receive two doses of either the test vaccine or the active control vaccine. Varicella-zoster virus (VZV) antibody was detected before vaccination and 42 days after the two doses of vaccination.
RESULTS:
The lower limits of the 95% CI for the differences in seroconversion rates and geometric mean titer (GMT) ratios between the two groups were greater than their respective pre-set non-inferiority margins. The overall incidence of Adverse events (AEs) and adverse reactions (ARs) in the test group was significantly lower than those in the control group. Additionally, the incidence rates of swelling and fatigue were lower in the test group compared to the control group after vaccination.
CONCLUSIONS:
The test freeze-dried live attenuated VarV demonstrated good immunogenicity and higher safety compared to the active control vaccine in healthy participants aged 13-55 years.
CLINICAL TRIALS REGISTRATION:
www.clinicaltrials.gov identifier: NCT06592456.
2025-12-31Emerging Microbes & Infections
Exploring the standardization of human nasal antibody measurements
Article
作者: Xu, Miao ; Liu, Guanxing ; Wang, Ying ; He, Qian ; Fu, Yulong ; Liang, Zhenglun ; Chen, Si ; Mao, Qunying ; Li, Na ; Wang, Junzhi ; Zhang, Xuanxuan ; Wang, Zhongfang ; Chen, Ling ; Wang, Qian
Mucosal immunity is crucial for preventing the infection and transmission of respiratory viruses. Nasal antibody is inversely correlated with a lower risk of infection with respiratory viruses. However, the current reference standard for nasal antibody assessment is serum-based, mainly consisting of monomeric IgG and IgA. The applicability of serum-derived standards for assessing nasal antibodies, consisting mostly of dimeric or polymeric secretory IgA (sIgA), remains unvalidated. Herein, we first proved that the sera-derived standard was not applicable for assessing nasal antibodies. Using a non-homologous standard as a calibrator introduced systematic error up to 10 times, which did not benefit the understanding of mucosal antibody response. Therefore, we attempted to develop two candidate standards (CS1, CS2) using nasal mucosal lining fluids (NMLFs) collected from SARS-CoV-2 Omicron convalescents or intranasal vaccine recipients, and CS3 using a sIgA monoclonal antibody. CS2 exhibited broad-spectrum binding activity against 12 SARS-CoV-2 strains, including all tested Omicron subvariants. A collaborative study conducted by seven laboratories demonstrated that CS2 improved the harmonization of inter-laboratory variability (pre-standardization geometric coefficients of variance, 14-314%; post-standardization, 3-35%). Using CS2 ensured an accurate assessment of nasal antibodies. Thus, CS2 was established as a national standard for evaluating nasal SARS-CoV-2-specific antibodies (Lot: 300052-202401, 1000 U/mL). Our work provides a benchmark for evaluating mucosal vaccines for SARS-CoV-2 and inspires new avenues for developing new reference standards for other mucosal vaccines.
2025-12-31Human Vaccines & Immunotherapeutics
Immunogenicity and safety of a live attenuated varicella vaccine in children aged 1 to 12 years: A double-blind, randomized, parallel-controlled phase III clinical trial in China
Article
作者: Li, Jingxin ; Chu, Kai ; Zhang, Yang ; Sun, Jinfang ; Zhang, Hao ; Wang, Shiyuan ; Zhu, Fengcai ; Li, Guifan ; Shi, Jinhui ; Chang, Xianyun
Chickenpox outbreaks frequently occur in collective settings such as kindergartens and schools, posing a significant threat to children's physical and mental health. This study aimed to evaluate the immunogenicity and safety of the freeze-dried live attenuated varicella vaccine (VarV) developed by Beijing Minhai Biotechnology Co. LTD. in healthy participants aged 1-12 years. In this phase III, single-center, randomized, double-blind, active-controlled trial,1,200 healthy participants randomly assigned in a 1:1 ratio to receive one dose of either the test vaccine or the active control vaccine. Venous blood samples were collected before vaccination and 42 days after vaccination, and the fluorescent antibody to membrane antigen (FAMA) assay was used to detect VZV antibody. Adverse events (AEs) observed within 42 days after vaccination and serious adverse events (SAEs) within six months after vaccination were recorded. The seroconversion rates in the test and control groups were 96.79% and 96.43%, respectively, with a difference of 0.36% (95% CI, -1.76%-2.48%). The geometric mean titers (GMTs) were 61.74 and 58.04, respectively, with a difference of 1.06 (95% CI, 0.92-1.23). The lower limits of the 95% CI for the differences in seroconversion rates and GMT ratios between the two groups were greater than their respective pre-set non-inferiority margins. The overall incidence of AEs (p = .0112) in the test group was significantly lower than that in the control group. The freeze-dried live attenuated VarV developed by Beijing Minhai Biotechnology Co. LTD. demonstrated good immunogenicity and higher safety compared to the active control vaccine in healthy participants aged 1-12 years.
100 项与 深圳康泰生物制品股份有限公司 相关的药物交易
登录后查看更多信息
100 项与 深圳康泰生物制品股份有限公司 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年08月18日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
药物发现
3
16
临床前
临床申请
2
2
临床申请批准
临床1期
6
2
临床2期
临床3期
4
4
申请上市
批准上市
11
12
其他
登录后查看更多信息
当前项目
登录后查看更多信息
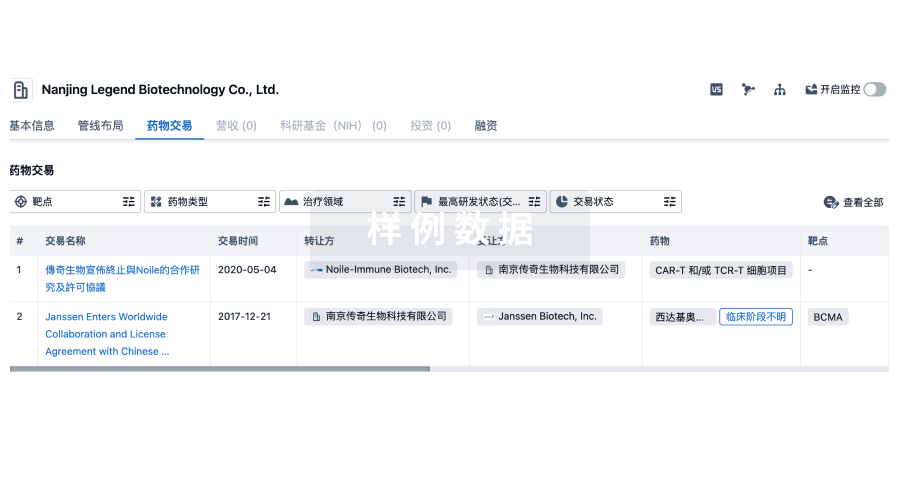
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
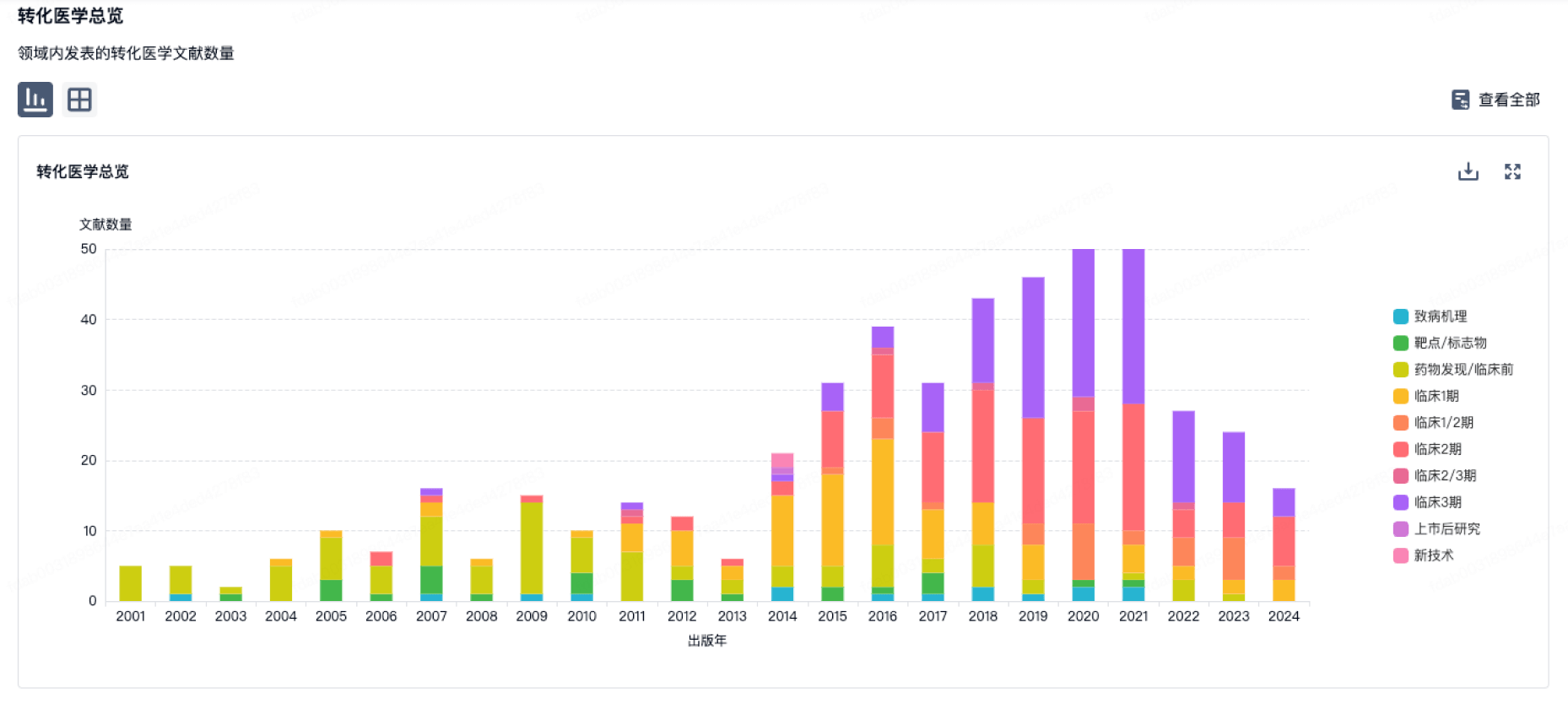
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
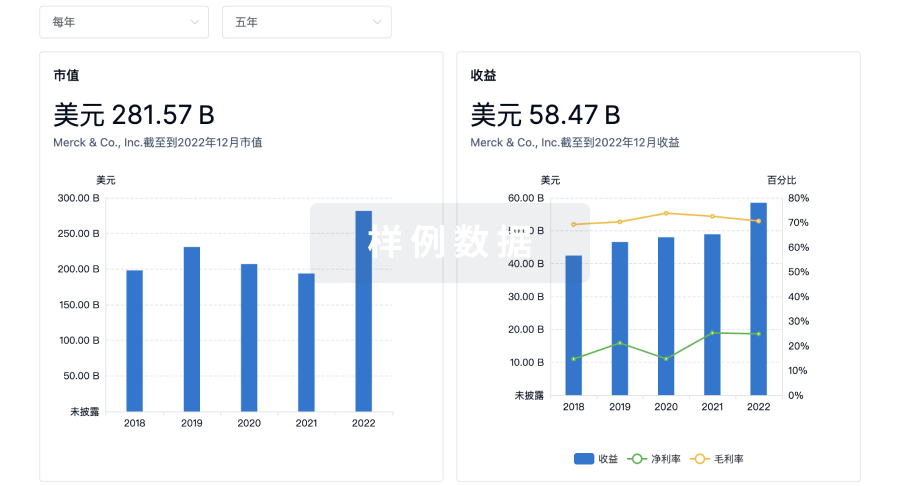
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用