预约演示
更新于:2025-01-23
ALK x BTK
更新于:2025-01-23
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
100 项与 ALK x BTK 相关的临床结果
登录后查看更多信息
100 项与 ALK x BTK 相关的转化医学
登录后查看更多信息
登录后查看更多信息
2024-12-01European Journal of Medicinal Chemistry
Discovery of orally bioavailable ALK PROTACs based ceritinib against ALK positive cancers
Article
作者: Liu, Zi ; Gong, Youling ; Luo, Yi ; Jie, Hui ; Chen, Yuanwei ; Pan, LiLi ; Xie, Yongmei ; Liu, Chengyali ; Tang, Kexin ; Zhou, Haoxuan ; Li, Yujue ; liu, scheZi ; Chen, Wei ; Hu, Mingxing
2023-02-07Biochemistry
Evaluation of a Pooling Chemoproteomics Strategy with an FDA-Approved Drug Library
Article
作者: Chen, Taosheng ; Chen, Ping-Chung ; Peng, Junmin ; Yang, Ka ; Sun, Huan ; Zhang, Xue ; Yarbro, Jay ; Wu, Zhiping ; Fu, Yingxue
2022-05-01Annals of Hematology
Epstein-Barr virus–positive diffuse large B-cell lymphoma after frontline brentuximab vedotin treatment of classical Hodgkin lymphoma
Letter
作者: Tse, Eric ; Loong, Florence ; Hwang, Yu-Yan ; Au-Yeung, Rex ; Kwong, Yok-Lam ; Chau, David
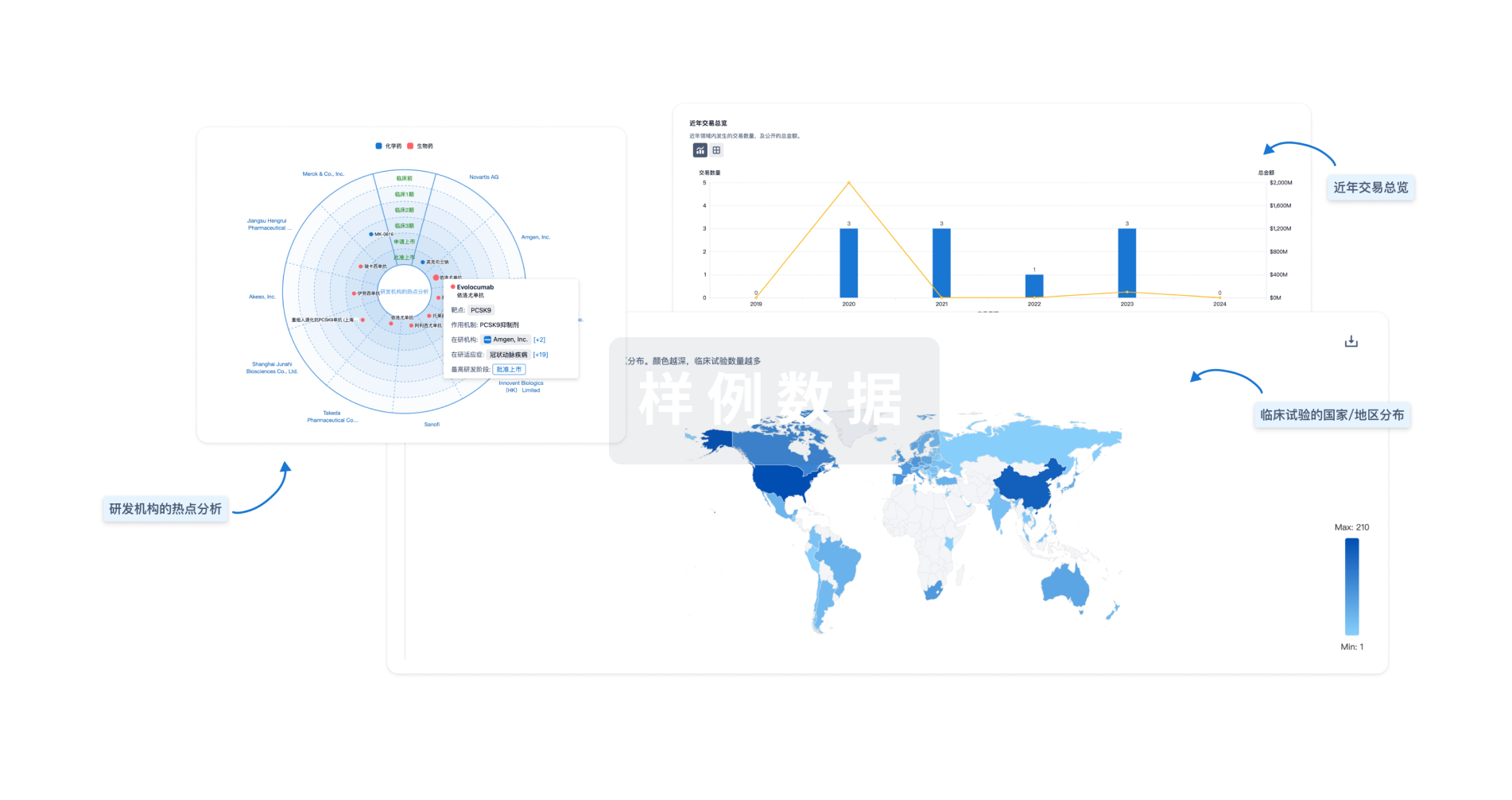
分析
对领域进行一次全面的分析。
登录
或
来和芽仔聊天吧
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用