预约演示
更新于:2025-08-29

Arog Pharmaceuticals, Inc.
更新于:2025-08-29
概览
标签
血液及淋巴系统疾病
肿瘤
小分子化药
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

NCT03258931
Phase III Randomized Study of Crenolanib Versus Midostaurin Administered Following Induction Chemotherapy and Consolidation Therapy in Newly Diagnosed Subjects With FLT3 Mutated Acute Myeloid Leukemia
NCT03324243
A Phase II Study of Crenolanib With Fludarabine and Cytarabine in Pediatric Patients With Relapsed/Refractory FLT3-Mutated Acute Myeloid Leukemia
NCT03193918
Phase I/Ib Study of Crenolanib With Ramucirumab and Paclitaxel as Second Line Therapy for Advanced Esophagogastric Adenocarcinoma
100 项与 Arog Pharmaceuticals, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2021-01-01Neuro-oncology advances
Phase I study using crenolanib to target PDGFR kinase in children and young adults with newly diagnosed DIPG or recurrent high-grade glioma, including DIPG
Article
作者: Patay, Zoltan ; Li, Xiaoyu ; Stewart, Clinton F ; Onar-Thomas, Arzu ; Zhang, Jinghui ; Gajjar, Amar ; Campagne, Olivia ; Wetmore, Cynthia ; Jain, Vinay ; Merchant, Thomas E ; Broniscer, Alberto ; Chiang, Jason ; Tinkle, Christopher L ; Orr, Brent A ; Baker, Suzanne J ; Huang, Jie
Abstract:
Background:
Platelet-derived growth factor receptor (PDGFR) signaling has been directly implicated in pediatric high-grade gliomagenesis. This study evaluated the safety and tolerability of crenolanib, a potent, selective inhibitor of PDGFR-mediated phosphorylation, in pediatric patients with high-grade glioma (HGG).
Methods:
We used a rolling-6 design to study the maximum tolerated dose (MTD) of once-daily crenolanib administered during and after focal radiation therapy in children with newly diagnosed diffuse intrinsic pontine glioma (DIPG) (stratum A) or with recurrent/progressive HGG (stratum B). Pharmacokinetics were studied during the first cycle at the first dose and at steady state (day 28). Alterations in PDGFRA were assessed by Sanger or exome sequencing and interphase fluorescence in situ hybridization or single nucleotide polymorphism arrays.
Results:
Fifty evaluable patients were enrolled in the 2 strata, and an MTD of 170 mg/m2 was established for both. Dose-limiting toxicities were primarily liver enzyme elevations and hematologic count suppression in both strata. Crenolanib AUC0–48h and CMAX did not differ significantly for crushed versus whole-tablet administration. Overall, PDGFRA alterations were observed in 25% and 30% of patients in stratum A and B, respectively. Neither crenolanib therapy duration nor survival outcomes differed significantly by PDGFRA status, and overall survival of stratum A was similar to that of historical controls.
Conclusions:
Children tolerate crenolanib well at doses slightly higher than the established MTD in adults, with a toxicity spectrum generally similar to that in adults. Studies evaluating intratumoral PDGFR pathway inhibition in biomarker-enriched patients are needed to evaluate further the clinical utility of crenolanib in this population.
2017-10-10Oncotarget
Crenolanib is a type I tyrosine kinase inhibitor that inhibits mutant KIT D816 isoforms prevalent in systemic mastocytosis and core binding factor leukemia
Article
作者: Haeusser, Lara A. ; Illing, Barbara ; Kampa-Schittenhelm, Kerstin Maria ; Schittenhelm, Marcus Matthias ; Blumenstock, Gunnar ; Pavlovsky, Ashly A. ; Frey, Julia
Activating D816 mutations of the class III receptor tyrosine kinase KIT are associated with the majority of patients with systemic mastocytosis (SM), but also core binding factor (CBF) AML, making KIT mutations attractive therapeutic targets for the treatment of these cancers. Crenolanib is a potent and selective inhibitor of wild-type as well as mutant isoforms of the class III receptor tyrosine kinases FLT3 and PDGFRα/β. Notably, crenolanib inhibits constitutively active mutant-FLT3 isoforms resulting from amino acid substitutions of aspartic acid at codon 835, which is homologous to codon 816 in the KIT gene - suggesting sensitivity against mutant-KIT D816 isoforms as well. Here we demonstrate that crenolanib targets KIT D816 in SM and CBF AML models: crenolanib inhibits cellular proliferation and initiates apoptosis of mastocytosis cell lines expressing these mutations. Target-specificity was confirmed using an isogenic cell model. In addition, we demonstrate that KIT D816 mutations are targetable with clinically achievable doses of crenolanib. Further, a rationale to combine cladribine (2-CDA), the therapeutic standard in SM, with crenolanib is provided. In conclusion, we demonstrate that crenolanib is an inhibitor of mutant-KIT D816 isoforms at clinically achievable concentrations, and thus may be a potential treatment for SM and CBF AML as a monotherapy or in combination approaches.
2015-08-01Gastroenterology1区 · 医学
Platelet-Derived Growth Factor Receptor-α Regulates Proliferation of Gastrointestinal Stromal Tumor Cells With Mutations in KIT by Stabilizing ETV1
1区 · 医学
Article
作者: Bardsley, Michael R ; Ordog, Tamas ; Ramachandran, Abhijit ; Gajdos, Gabriella B ; Tang, Chih-Min ; Hayashi, Yujiro ; Gibbons, Simon J ; Milosavljevic, Srdjan ; Farrugia, Gianrico ; Bingener-Casey, Juliane ; Fletcher, Jonathan A ; Sicklick, Jason K ; Reid-Lombardo, K Marie ; Rubin, Brian P ; Choi, Kyoung Moo ; Taguchi, Takahiro ; Toyomasu, Yoshitaka ; Kendrick, Michael L ; Gupta, Anu
BACKGROUND & AIMS:
In gastrointestinal muscles, v-kit Hardy-Zuckerman 4 feline sarcoma viral oncogene homolog (KIT) is predominantly expressed by interstitial cells of Cajal (ICC) and platelet-derived growth factor receptor-α (PDGFRA) polypeptide is expressed by so-called fibroblast-like cells. KIT and PDGFRA have been reported to be coexpressed in ICC precursors and gastrointestinal stromal tumors (GISTs), which originate from the ICC lineage. PDGFRA signaling has been proposed to stimulate growth of GISTs that express mutant KIT, but the effects and mechanisms of selective blockade of PDGFRA are unclear. We investigated whether inhibiting PDGFRA could reduce proliferation of GIST cells with mutant KIT via effects on the KIT-dependent transcription factor ETV1.
METHODS:
We studied 53 gastric, small intestinal, rectal, or abdominal GISTs collected immediately after surgery or archived as fixed blocks at the Mayo Clinic and University of California, San Diego. In human GIST cells carrying imatinib-sensitive and imatinib-resistant mutations in KIT, PDGFRA was reduced by RNA interference (knockdown) or inhibited with crenolanib besylate (a selective inhibitor of PDGFRA and PDGFRB). Mouse ICC precursors were retrovirally transduced to overexpress wild-type Kit. Cell proliferation was analyzed by methyltetrazolium, 5-ethynyl-2'-deoxyuridine incorporation, and Ki-67 immunofluorescence assays; we also analyzed growth of xenograft tumors in mice. Gastric ICC and ICC precursors, and their PDGFRA(+) subsets, were analyzed by flow cytometry and immunohistochemistry in wild-type, Kit(+/copGFP), Pdgfra(+/eGFP), and NOD/ShiLtJ mice. Immunoblots were used to quantify protein expression and phosphorylation.
RESULTS:
KIT and PDGFRA were coexpressed in 3%-5% of mouse ICC, 35%-44% of ICC precursors, and most human GIST samples and cell lines. PDGFRA knockdown or inhibition with crenolanib efficiently reduced proliferation of imatinib-sensitive and imatinib-resistant KIT(+)ETV1(+)PDGFRA(+) GIST cells (50% maximal inhibitory concentration = 5-32 nM), but not of cells lacking KIT, ETV1, or PDGFRA (50% maximal inhibitory concentration >230 nM). Crenolanib inhibited phosphorylation of PDGFRA and PDGFRB, but not KIT. However, Kit overexpression sensitized mouse ICC precursors to crenolanib. ETV1 knockdown reduced KIT expression and GIST proliferation. Crenolanib down-regulated ETV1 by inhibiting extracellular-signal-regulated kinase (ERK)-dependent stabilization of ETV1 protein and also reduced expression of KIT and PDGFRA.
CONCLUSIONS:
In KIT-mutant GIST, inhibition of PDGFRA disrupts a KIT-ERK-ETV1-KIT signaling loop by inhibiting ERK activation. The PDGFRA inhibitor crenolanib might be used to treat patients with imatinib-resistant, KIT-mutant GIST.

100 项与 Arog Pharmaceuticals, Inc. 相关的药物交易
登录后查看更多信息
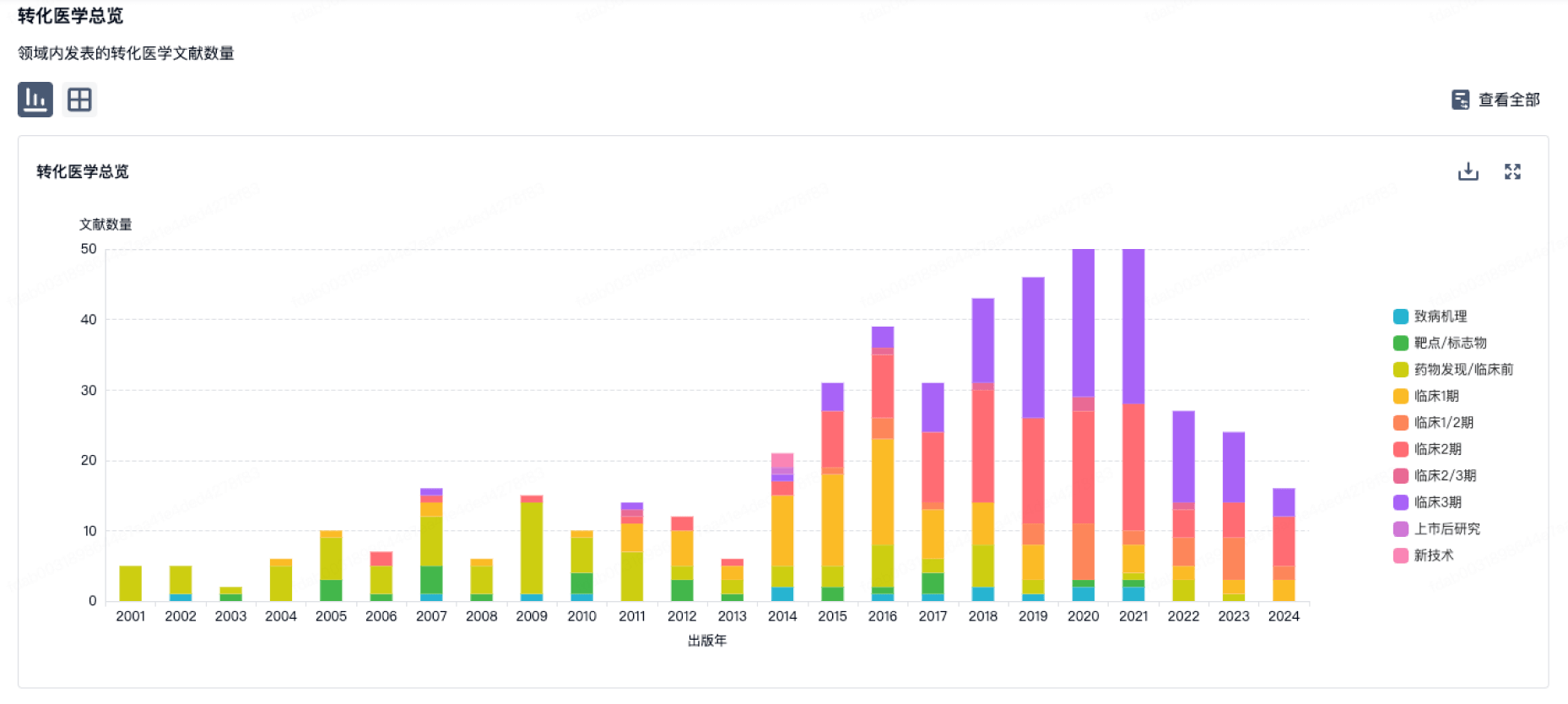
100 项与 Arog Pharmaceuticals, Inc. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年09月01日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
临床3期
1
登录后查看更多信息
当前项目
登录后查看更多信息
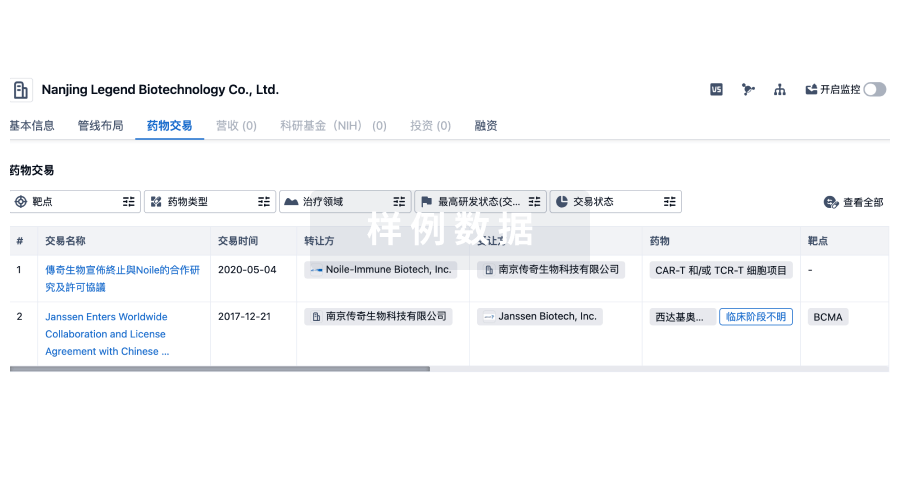
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
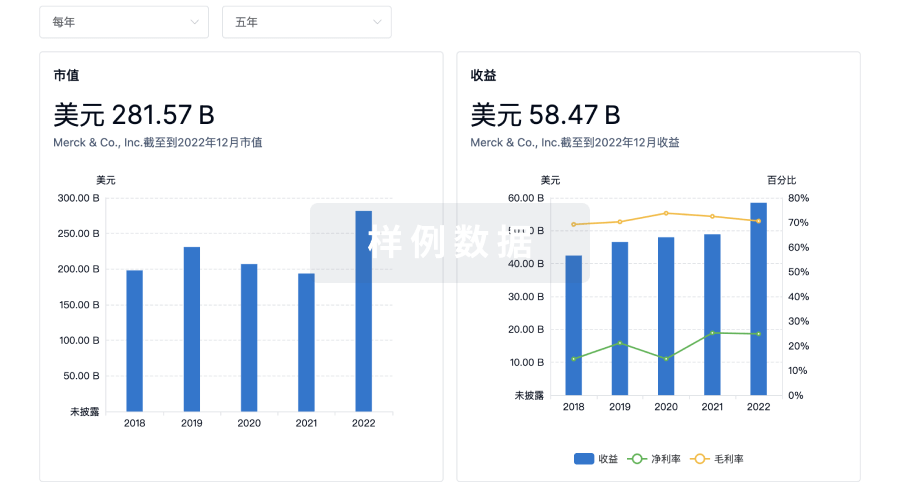
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用