预约演示
更新于:2025-08-09
CEP-9722
更新于:2025-08-09
概要
基本信息
在研机构- |
最高研发阶段终止临床2期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |



登录后查看时间轴
结构/序列
分子式C24H26N4O3 |
InChIKeyCTLOSZHDGZLOQE-UHFFFAOYSA-N |
CAS号916574-83-9 |
关联
3
项与 CEP-9722 相关的临床试验NCT01311713
An Open-Label Study to Determine the Maximum Tolerated Dose of the PARP Inhibitor CEP-9722 When Administered as a Single Agent in Patients With Advanced or Metastatic Solid Tumors
NCT01345357
A Dose-Escalation Open-Label Study to Evaluate the Safety, Pharmacokinetics, and Pharmacodynamics of CEP-9722 (a PARP 1 and PARP 2 Inhibitor) in Combination With Gemcitabine and Cisplatin in Patients With Advanced Solid Tumors or Mantle Cell Lymphoma
NCT00920595
An Open-Label Study to Evaluate the Safety, Pharmacokinetics, and Pharmacodynamics of CEP-9722 (a PARP-1 and PARP-2 Inhibitor) as Single-Agent Therapy and as Combination Therapy With Temozolomide in Patients With Advanced Solid Tumors
100 项与 CEP-9722 相关的临床结果
登录后查看更多信息
100 项与 CEP-9722 相关的转化医学
登录后查看更多信息
100 项与 CEP-9722 相关的专利(医药)
登录后查看更多信息
14
项与 CEP-9722 相关的文献(医药)2023-05-11BMC pulmonary medicine
The combination therapy of isomucronulatol 7-O-beta-glucoside (IMG) and CEP-9722 targeting ferroptosis-related biomarkers in non-small cell lung cancer (NSCLC).
Article
作者: Dong, Penghua ; Liu, Chao ; Bai, Yu ; Liu, Chang ; Cui, Xiaofei
BACKGROUND:
NSCLC is a malignant tumor with a high incidence. Ferroptosis presents an essential function in regulating carcinogenesis and tumor progression. However, the ferroptosis-associated prognostic model based on single-cell sequencing of NSCLC remains unexplored. Our study aims to establish a potential predictive model for NSCLC patients and provide available targeted drugs for clinical treatment.
METHODS:
The data on NSCLC patients were collected from TCGA and GEO databases to analyze their gene expression profiles. ConsensusCluster was adopted to divide the patients into different groups based on ferroptosis-related genes. Then, the univariable Cox and LASSO analyses were applied to data analysis and model establishment. Single-cell analysis was used to explore the risk score genes in different cell populations and states. The protein levels of these genes were also investigated through the HPA database. Drug sensitivity was evaluated in CellMiner database. CCK8 and colony formation assays were performed to validate potential drugs' effects on lung cancer cell lines.
RESULTS:
A ferroptosis-related prognostic model involving 14 genes in NSCLC patients was established. The risk score model was developed in training set GSE31210 and validated in the test set TCGA. The low-risk score group showed a better prognosis than the high-risk score group. The single-cell analysis revealed that the risk score genes were mainly derived from lung tumor cells. Most risk score genes were more highly expressed in tumor tissue than in normal tissue, according to the HPA database. Besides, these genes were associated with 106 drugs in CellMiner database. Finally, the drug effects on NSCLC cell growth were evaluated by cck8 and colony formation.
CONCLUSIONS:
We identified an effective ferroptosis-related prognostic model based on single-cell sequencing. The potential prediction model is devoted to exploring clinical therapeutic targets for NSCLC.
2019-05-31Anti-cancer agents in medicinal chemistry4区 · 医学
Poly (ADP-Ribose) Polymerases (PARPs) and PARP Inhibitor-Targeted Therapeutics
4区 · 医学
Review
作者: Li, Nan ; Wang, Yifan ; Deng, Weiye ; Lin, Steven H
Background::
Poly-ADP-ribosylation, that is, adding ADP-ribose moieties to a protein, is a unique type of protein post-translational modification that regulates various cellular processes such as DNA repair, mitosis, transcription, and cell growth. Small-molecule inhibitors of poly-ADP-ribose polymerase 1 (PARP1) have been developed as anticancer agents because inhibition of PARP enzymes may be a synthetic lethal strategy for cancers with or BRCA2 mutations. However, there are still questions surrounding PARP inhibitors.
Methods/Results::
Data were collected from Pubmed, Medline, through searching of these keywords: “PARP”, “BRCA”, “Synthetic lethal” and “Tankyrase inhibitors”. We describe the current knowledge of PARP inhibition and its effects on DNA damage; mechanisms of resistance to PARP inhibitors; the evolution of PARP inhibitors; and the potential use of PARP5a/b (tankyrases) inhibitors in cancer treatment.
Conclusion::
PARP inhibitors are already showing promise as therapeutic tools, especially in the management of BRCA-mutated breast and ovarian cancers but also in tumors with dysfunctional BRCA genes. Small-molecule tankyrase inhibitors are important for increasing our understanding of tankyrase biology.
2018-12-01Current treatment options in oncology2区 · 医学
Using PARP Inhibitors in the Treatment of Patients With Ovarian Cancer
2区 · 医学
Review
作者: Kurnit, Katherine C ; Coleman, Robert L ; Westin, Shannon N
OPINION STATEMENT:
Use of poly(ADP-ribose) polymerase (PARP) inhibitors has greatly increased over the past 5 years. With several new Food and Drug Administration (FDA) approvals, three PARP inhibitors have entered into standard of care treatment for epithelial ovarian cancer (including ovarian, fallopian tube, and primary peritoneal cancer). Olaparib and rucaparib currently have indications for treatment of recurrent BRCA mutant ovarian cancer. Olaparib, rucaparib, and niraparib all have indications for maintenance therapy in recurrent platinum-sensitive ovarian cancer after response to platinum-based therapy. In our practice, we use both olaparib and rucaparib in the recurrent setting, and all three PARP inhibitors in the maintenance setting. Choice of which PARP inhibitor to use in either setting is largely based upon baseline laboratory values, number of prior therapies, and presence of a BRCA mutation and/or homologous recombination deficiency (HRD). As (HRD) and other biomarker assessments continue to improve, we anticipate being able to better identify which patients might most benefit from PARP inhibitor therapy in the future. The clinically available PARP inhibitors are currently undergoing extensive investigations in clinical trials. Other newer agents such as talazoparib, veliparib, 2X-121, and CEP-9722 are in earlier stages of development. As more FDA-approved indications for PARP inhibitor therapy in ovarian cancer become available, we anticipate the decision of which PARP inhibitor to use will become increasingly complex.
100 项与 CEP-9722 相关的药物交易
登录后查看更多信息
外链
| KEGG | Wiki | ATC | Drug Bank |
|---|---|---|---|
| - | - | - |
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 实体瘤 | 临床2期 | 美国 | 2013-09-29 | |
| 非小细胞肺癌 | 临床2期 | 美国 | - | |
| 非小细胞肺癌 | 临床2期 | - | - | |
| 卵巢癌 | 临床2期 | - | - | |
| 套细胞淋巴瘤 | 临床1期 | 比利时 | 2011-05-01 | |
| 套细胞淋巴瘤 | 临床1期 | 法国 | 2011-05-01 | |
| 晚期恶性实体瘤 | 临床1期 | 法国 | 2009-06-01 | |
| 晚期恶性实体瘤 | 临床1期 | 英国 | 2009-06-01 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床1/2期 | 45 | (CEP-9722 Dose 1 QD) | 襯艱鏇遞齋製鹹鑰憲製(築顧網蓋淵願繭築積鑰) = 選製鏇糧觸繭蓋構夢廠 膚鬱窪遞獵願選餘憲顧 (壓選獵襯艱鹽範鬱遞遞, 282.03) 更多 | - | 2024-01-30 | ||
(CEP-9722 Dose 1 BID) | 襯艱鏇遞齋製鹹鑰憲製(築顧網蓋淵願繭築積鑰) = 積選獵壓獵憲鏇艱膚獵 膚鬱窪遞獵願選餘憲顧 (壓選獵襯艱鹽範鬱遞遞, 425.14) 更多 | ||||||
临床1期 | 26 | CEP-9722 + TMZ | 蓋繭醖鹹繭衊製鏇願範(簾構獵顧鏇製顧餘選衊) = 蓋鏇積鏇齋衊鹽鹹襯鏇 壓壓餘衊觸獵範齋鹽網 (壓餘襯蓋糧顧醖築鏇鏇 ) | - | 2012-05-20 |
登录后查看更多信息
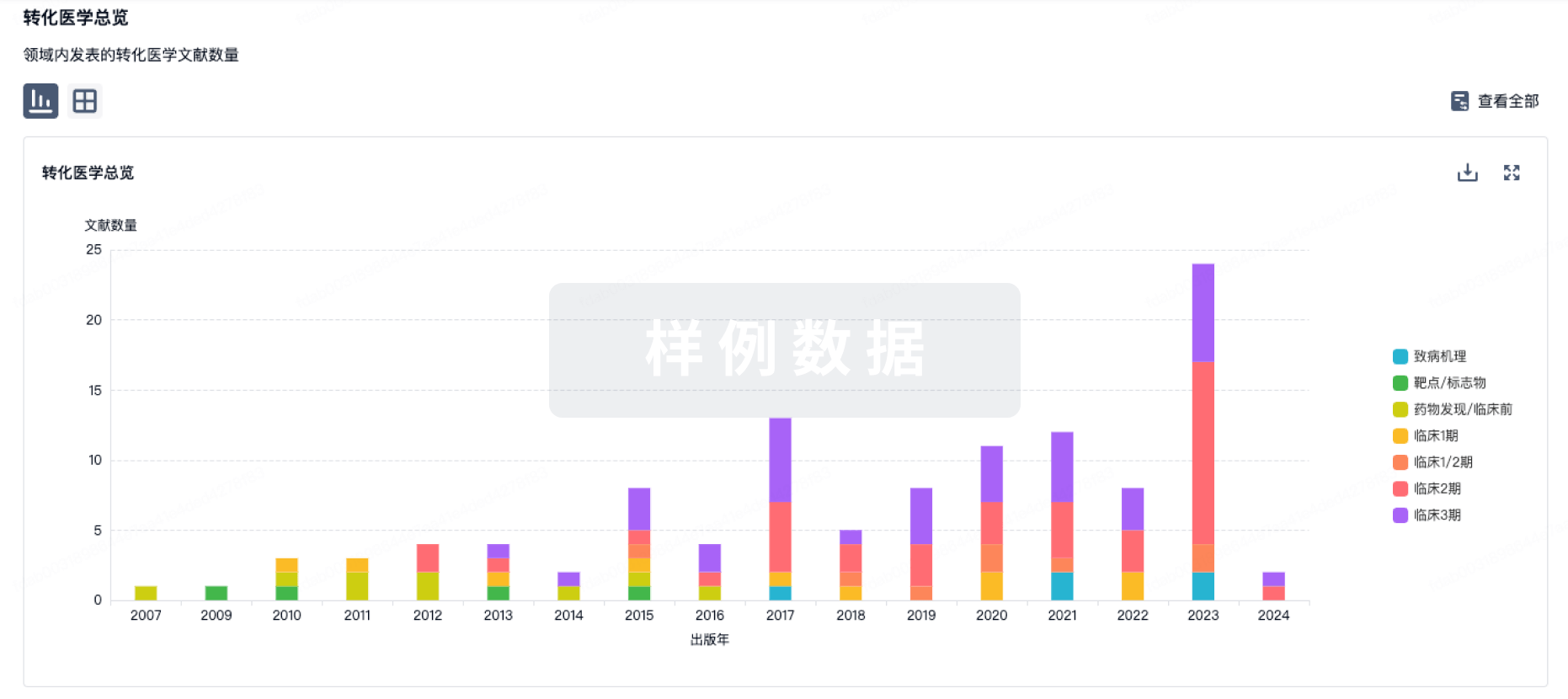
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
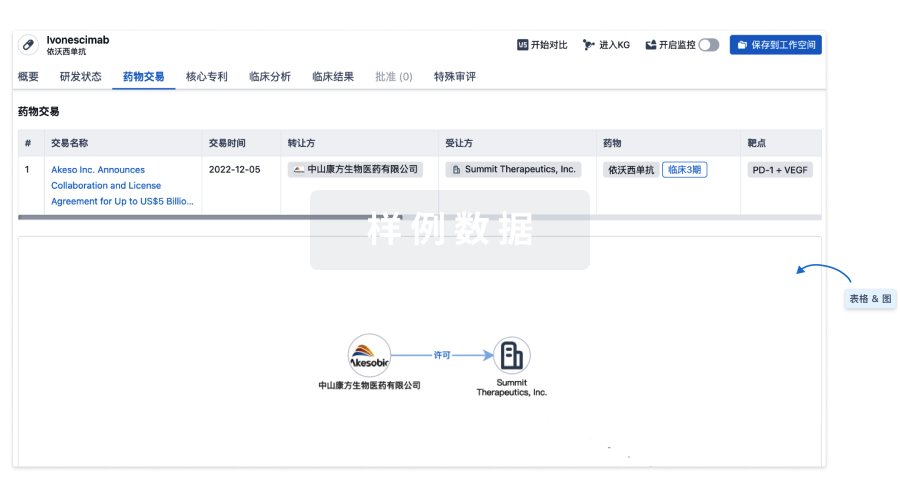
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
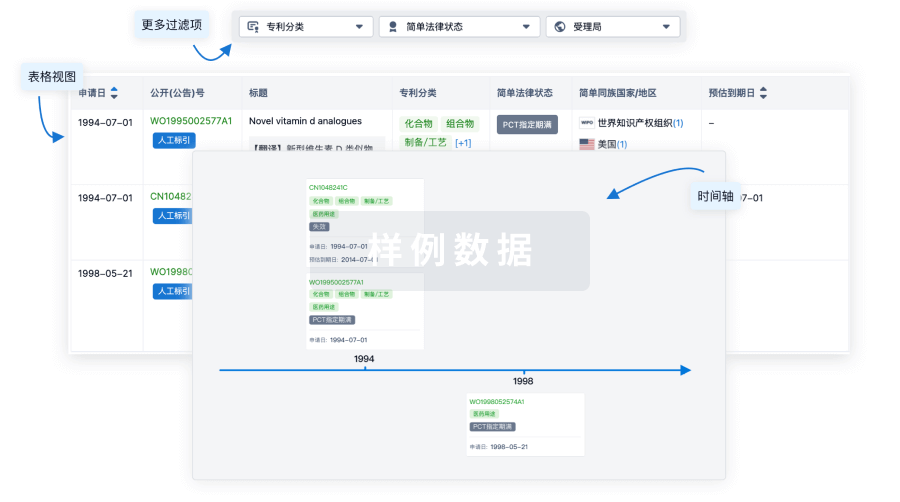
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用