预约演示
更新于:2025-05-07
Enterobacter Infection
肠杆菌感染
更新于:2025-05-07
基本信息
别名 Enterobacter infection、Enterobacter infections、Infection caused by Enterobacter + [4] |
简介- |
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |

EUCTR2019-001618-41-GB
FERARO: A prospective, randomised placebo controlled feasibility trial of Faecal microbiota Transplant to ERadicate gastrointestinal carriage of Antibiotic Resistant Organisms - FERARO
NCT04146922
Switch to Oral Antibiotics in Gram-negative Bacteremia (SOAB); a Randomized, Open-label, Clinical Trial.

EUCTR2013-004838-15-ES
Intestinal colonization by multiresistant enterobacteria in patients with kidney and liver transplantation: multicentre cohort study and randomized, controlled, open clinical trial. - Intestinal colonization by multiresistant enterobacteria in SOT
100 项与 肠杆菌感染 相关的临床结果
登录后查看更多信息
100 项与 肠杆菌感染 相关的转化医学
登录后查看更多信息
登录后查看更多信息
2025-04-01Virology
vB_Ent31 bacteriophage may combat Enterobacter cloacae infections with macrophage modulating activity
Article
作者: Li, Hong ; Tang, Yanqiong ; Li, Mengyuan ; Liu, Zhu ; Li, Juanjuan ; Zheng, Naijin ; Chi, Xue ; Ma, Xiang ; Feng, Xiaoshuang ; Ma, Jiayue
2025-02-01The Lancet Infectious Diseases
REVISITing treatment of metallo-β-lactamases
Article
作者: McCreary, Erin K ; Heil, Emily L
2024-11-01Microbes and Infection
miR-190 restores the innate immune homeostasis of Drosophila by directly inhibiting Tab2 in Imd pathway
Article
作者: Jin, Ping ; Zhu, Canhe ; Yang, Shangmin ; Wu, Jing ; Ma, Fei ; He, Yuqing ; Yao, Xiaolong
2022-07-04
免疫疗法合作并购
2022-06-21
并购创新药合作抗体
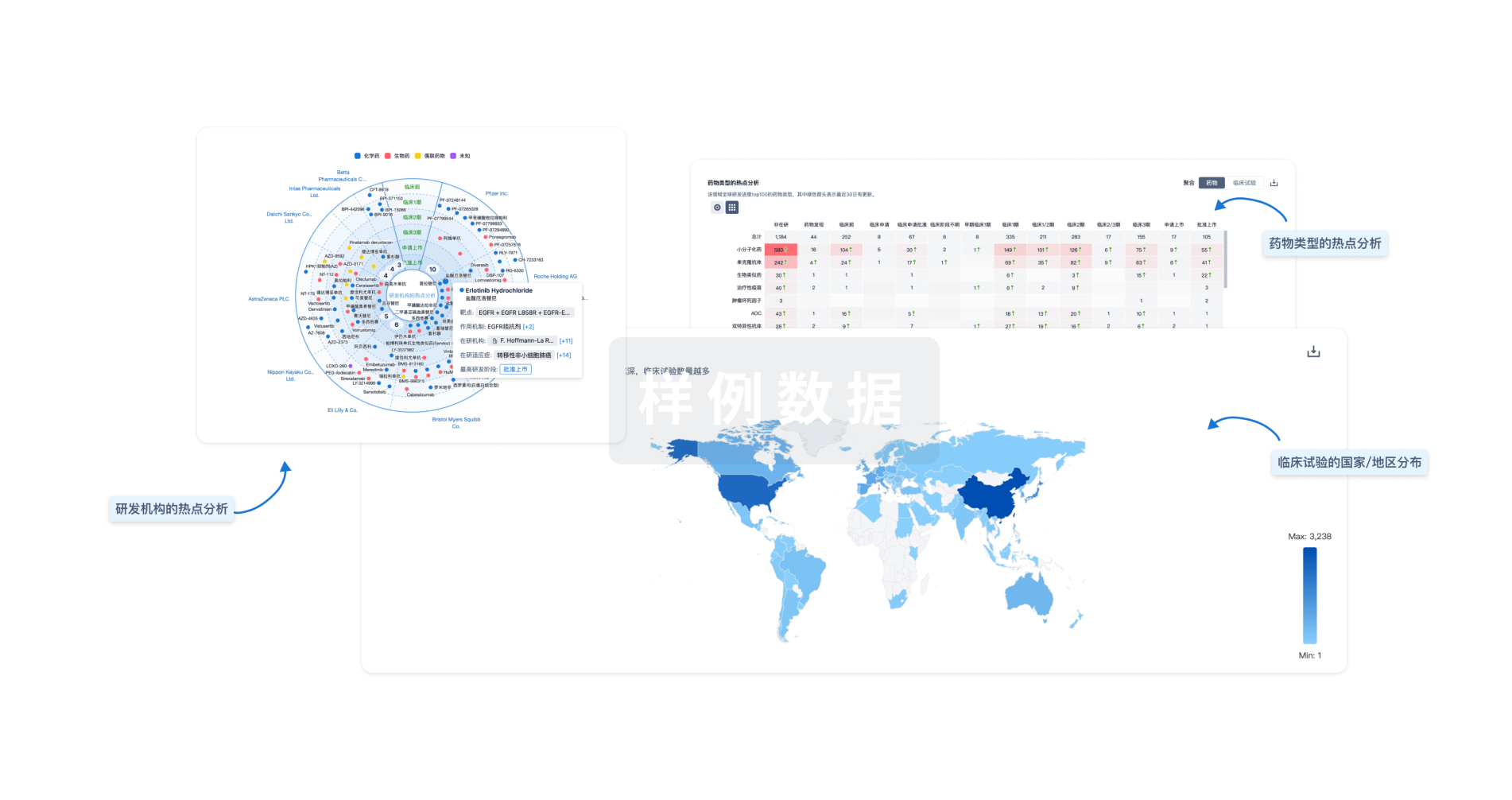
分析
对领域进行一次全面的分析。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用