预约演示
更新于:2025-05-07

NHS Lanarkshire
更新于:2025-05-07
概览
关联
NCT06928285
Community Rollout of Technology Enriched Rehabilitation After Stroke: An Implementation Study

NCT06908148
SALACIA: Randomised Control Trial of SALvesAn Neutral Electrolysed Water Versus Conventional Management of Non-healing dIAbetic Foot Wounds
NCT06114732
Motivating Physical Activity With Behavioural interVention and Electrical Stimulation Remotely in People With Intermittent Claudication (MAvERIC): a Feasibility Randomised Controlled Trial
100 项与 NHS Lanarkshire 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-04-21Neuropsychological Rehabilitation
The reliability and validity of brief cognitive screening tools used in traumatic brain injury: A systematic review
Review
作者: Fradera, Alexander ; Cullen, Breda ; McLaren, Jessica
2024-09-09British Journal of Surgery
SP3.1 - Could shorter length of stay and oncological non inferiority justify a radical paradigm shift towards RAS to be the gold standard for all rectal cancer resections
作者: Qazalbash, Zeeshan Ali ; Tan, Chin ; Mukherjee, Arijit ; Khan, Junaid ; Khopekar, Faid
2024-09-09British Journal of Surgery
ThP1.3 - Oncoplastic Surgery and Magseed Markers: A five-year snapshot of ambition and evolution in breast conserving surgery
作者: Murphy, Dermot ; Lannigan, Alison ; McIlhenny, Jennifer ; Lang, Anne ; Bell, Emma ; Gray, Karen
100 项与 NHS Lanarkshire 相关的药物交易
登录后查看更多信息
100 项与 NHS Lanarkshire 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年07月15日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
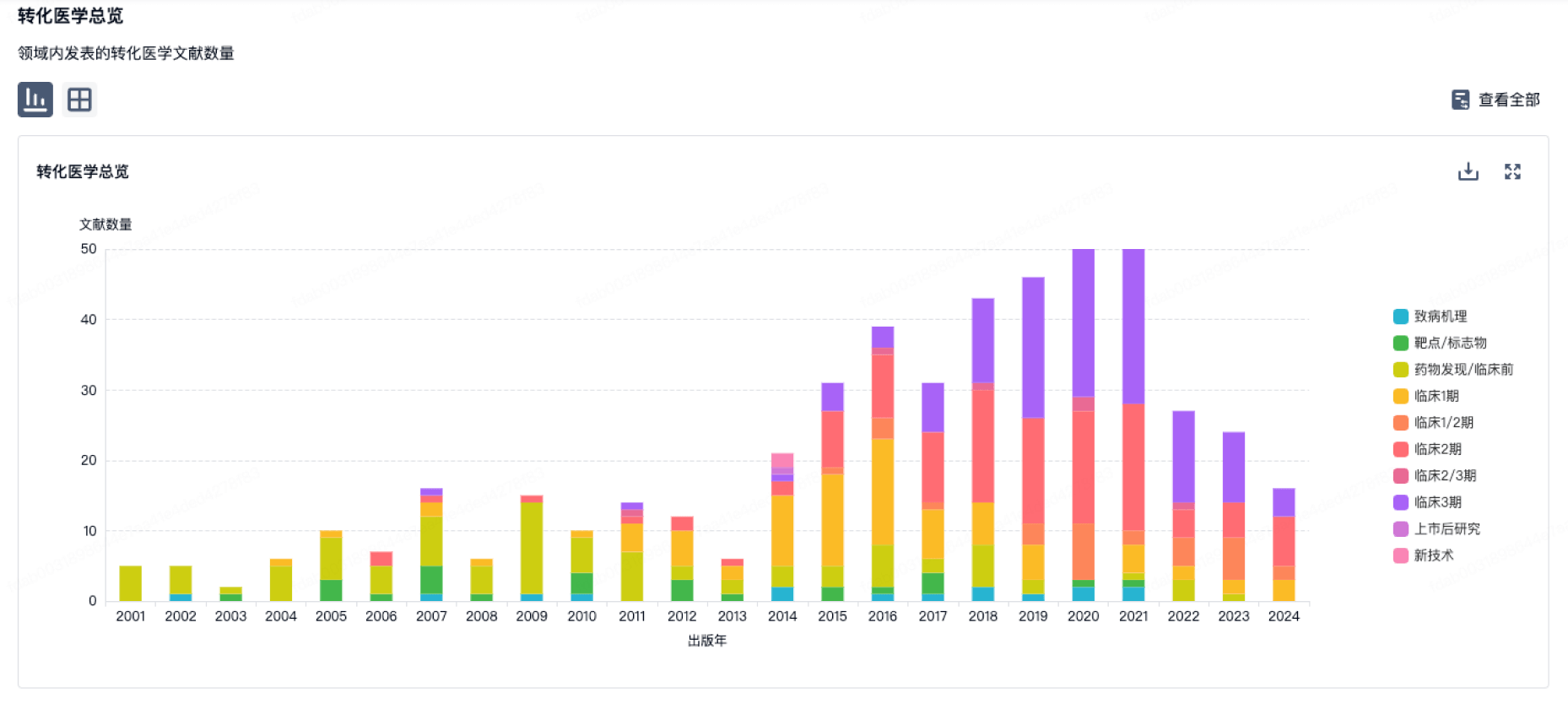
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
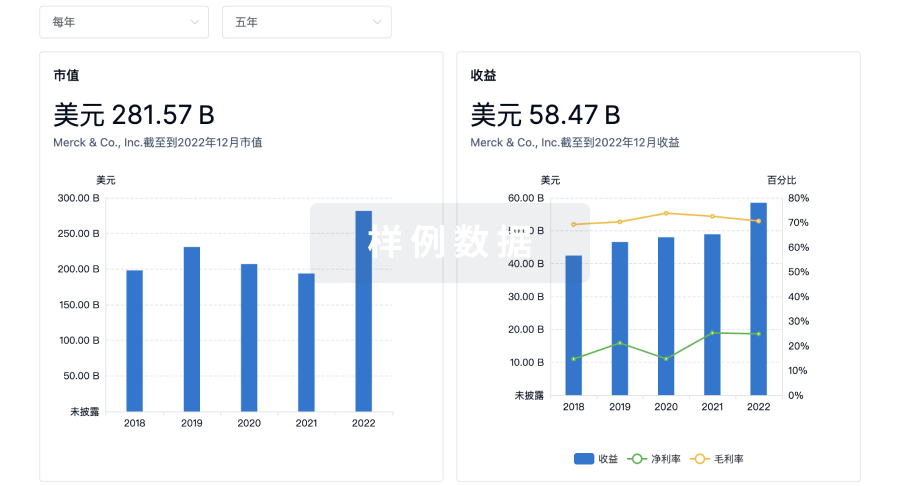
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用