预约演示
更新于:2025-08-14

MiMedx Group, Inc.
更新于:2025-08-14
概览
关联
NCT06600724
A Multicenter, Prospective, Randomized Controlled Modified Platform Trial Evaluating PURION Processed Lyophilized Human Amnion/Chorion Membrane (ppLHACM) and Standard of Care Versus Standard of Care Alone in the Treatment of Nonhealing Diabetic Foot Ulcers
NCT06560502
A Multicenter, Prospective, Randomized Controlled Modified Multi-Platform (Matriarch) Trial Evaluating Several Cellular, Acellular, and Matrix-like Products (CAMPs) and Standard of Care Versus Standard of Care Alone in the Management of DFUs and VLUs.

NCT06236750
A Post-Marketing Surveillance to Observe the Safety and Efficacy of Dehydrated Human Amnion/Chorion Membrane (DHACM) Wound Graft in the Management of Non-Ischemic Chronic Wounds
100 项与 MiMedx Group, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-03-02Journal of Wound Care
Clinical outcomes of lyophilised human amnion/chorion membrane in treatment of hard-to-heal diabetic foot ulcers in complex cases: a case series
Article
作者: Oltmann, Megan ; Forsyth, R Allyn ; Shahbazi, Sara ; Kyle, David ; Devlin, Carol ; Gilbert, Thomas J
Objective::
Diabetic foot ulcers (DFUs) are a common and severe complication of diabetes, characterised by high morbidity, recurrence and risk of amputation. Hard-to-heal (chronic) DFUs often fail to respond to standard of care (SoC), necessitating advanced interventions. Lyophilised human amnion/chorion membrane (LHACM) is a trilayer placental allograft that provides extracellular matrix support, growth factors and anti-inflammatory properties to promote wound closure. This case series evaluates the effectiveness of LHACM as an adjunct to SoC in treating hard-to-heal DFUs unresponsive to conventional treatments.
Method::
Patients with Wagner Grade 2 or 3 DFUs (each of which had been hard-to-heal and unresponsive to SoC for 1–3 years) and multiple comorbidities were treated with LHACM following thorough wound debridement, customised dressings and offloading strategies. Wound closure, infection control and functional outcomes were assessed.
Results::
This was a case series of three male patients, aged 65–66 years. All wounds demonstrated significant size reduction within three weeks of treatment, achieving complete closure within a mean of 47 days (range: 35–56 days). No infection recurrences or complications were observed and patients resumed daily activities. LHACM's ease of application and compatibility with SoC facilitated integration into the treatment protocol.
Conclusion::
LHACM demonstrated effectiveness in accelerating wound closure in complex hard-to-heal DFUs resistant to SoC, highlighting its potential to mitigate complications, reduce healthcare costs and improve patient quality of life. Further large scale studies are warranted to confirm these findings and explore broader applications in advanced wound care.
2024-12-02Journal of Wound Care
The impact of dual-enrolee (Medicare/Medicaid) status on venous leg ulcer outcomes: a retrospective study
Article
作者: De Jong, Julie L ; Kelso, Martha R ; Forsyth, R Allyn ; Wahab, Naz ; Hubbs, Brandon ; Tettelbach, William H ; Oropallo, Alisha ; Driver, Vickie
Objective::
To quantify race, sex, comorbidities, Medicaid status, and compare health outcomes for Medicare-only versus Medicare/Medicaid dual-enrolees who developed a hard-to-heal venous leg ulcer (VLU).
Method::
Medicare Limited Data Standard analytic hospital inpatient and outpatient department files were used to follow episodes of medical care for a VLU from 1 October 2015–2 October 2019. In an earlier study, patients diagnosed concurrently with chronic venous insufficiency and a VLU were propensity-matched. In this current work, cohorts were split into patients enrolled in Medicare-only and those enrolled in Medicare and Medicaid (dual-enrolees). Treatment methods were compared and the most commonly used cellular, acellular and matrix-like product (CAMP) among Medicare beneficiaries—dehydrated human amnion chorion membrane (DHACM)—was evaluated. Episode claims were used to document demographics, comorbidities and treatments of Medicare enrolees who developed VLUs and outcomes such as time to ulcer closure, rates of complications and hospital usage rates. Quality of life (QoL) metrics, such as pain and time to VLU closure, were compared across the groups.
Results::
Of the 555,284 Medicare beneficiaries evaluated in this analysis, 27% were Medicare/Medicaid dual-enrolees and 73% were Medicare-only enrolees. To qualify for Medicaid, patient income had to be ≤133% of the federal poverty level. Only 3% of Medicare-only patients and 6% of dual-enrolees had an Advantage plan, a lower rate than the general Medicare population. Dual-enrolees, compared to those covered by Medicare-only, demonstrated: a Charlson Comorbidity Index (CCI) score one point greater (p<0.0001); a higher percentage (16%) of patients from minority ethnic backgrounds; and significantly higher rates of emergency department visits (p<0.0001) and cellulitis (p=0.034). Dual-enrolees who received early and regularly applied CAMPs also reduced their treatment time by 21 days (p=0.0027), all of which can impact costs.
Conclusion::
The socioeconomic status of dual-enrolees included near poverty status, a higher percentage of patients from a minority ethnic background, and high rates of comorbidities compared to their Medicare-only counterparts. The VLUs of dual-enrolees took longer to close, developed more complications, and used significantly more hospital resources and expenses. Outcomes significantly improved when VLU episodes were treated with a CAMP, such as DHACM, while following parameters for use. Socioeconomic variables are associated with poor outcomes for patients with hard-to-heal (chronic) wounds. This should be tracked to find cost-effective interventions throughout their journey to provide equitable care and ensure they are not left behind. Greater access for dual-enrolees to CAMPs has the potential to improve clinical outcomes and patient QoL, while concomitantly reducing overall healthcare expenditure.
2024-10-02Journal of Wound Care
Experiences of patients with hard-to-heal wounds: insights from a pilot survey
Article
作者: Forsyth, R Allyn ; Wahab, Naz
Objective::
To learn about the experiences of people who seek treatment for hard-to-heal wounds, we distributed a nationwide pilot survey, asking questions about the nature of their wound, how it shaped their daily lives, pathways to receiving care and experiences with treatment. The long-term objective is to quantify the journey of patients with hard-to-heal wounds to identify ideal intervention points that will lead to the best outcomes. This article summarises the findings, implications, limitations and suggestions for future research.
Method::
Qualitative data were self-reported from patients with hard-to-heal wounds (open for ≥4 weeks) in a pilot chatbot survey, (Wound Expert Survey (WES)) provided online in the US on Meta platforms (Facebook and Instagram) between 2021 and 2022.
Results::
The US national pilot survey attracted responses from 780 patients, 27 of whom provided a video testimonial. Some 57% of patients delayed treatment because they believed their wound would heal on its own, and only 4% saw a wound care specialist. Respondents reported the cost of care as the most frequent reason for not following all of a doctor's treatment recommendations. Queries regarding quality of life (QoL) revealed that more than half (65%) said they have negative thoughts associated with their wound at least every few days. Some 19% of respondents said their wound had an odour and, of them, 34% said odour had a major or severe negative impact on their self-confidence. Economically, nearly one-quarter of respondents said having a wound led to a drop in their total household income and 17% said their wound led to a change in their employment status.
Conclusion::
A national pilot survey of patients with hard-to-heal wounds revealed that many delay seeking professional assistance and only a small minority see a wound care specialist. Experiencing an ulcer, even for a few months, can have significant negative effects on a patient's QoL. Patients frequently had negative thoughts associated with their wound, and odour compounded these negative effects, leading to major or severe negative impacts on self-confidence. Households experienced a decline in income, due to both the direct reduction or loss of patient employment and the additional time spent by family members assisting in patient recovery. Thus, a variety of factors contribute to poor outcomes for patients with hard-to-heal wounds. To validate and extend these preliminary results, future surveys of patients with hard-to-heal wounds should focus on additional reasons patients do not seek professional help sooner. To improve health outcomes and QoL, assessment of patient socioeconomic variables should occur whenever wound closure stalls.
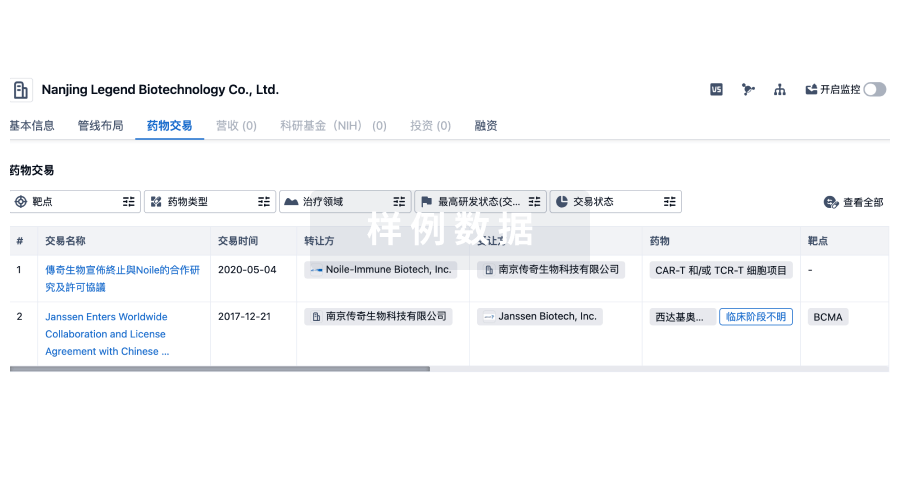
100 项与 MiMedx Group, Inc. 相关的药物交易
登录后查看更多信息
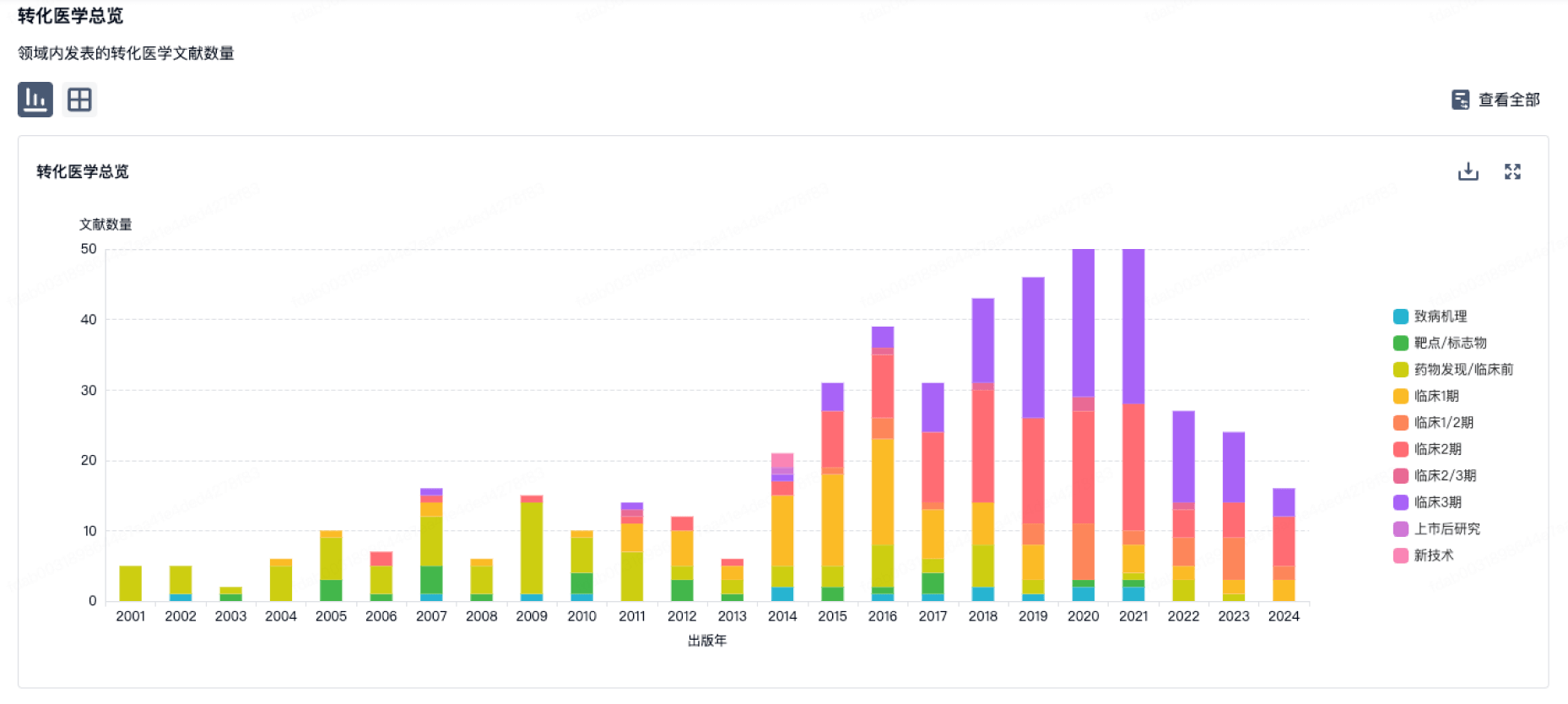
100 项与 MiMedx Group, Inc. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年08月24日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
其他
2
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
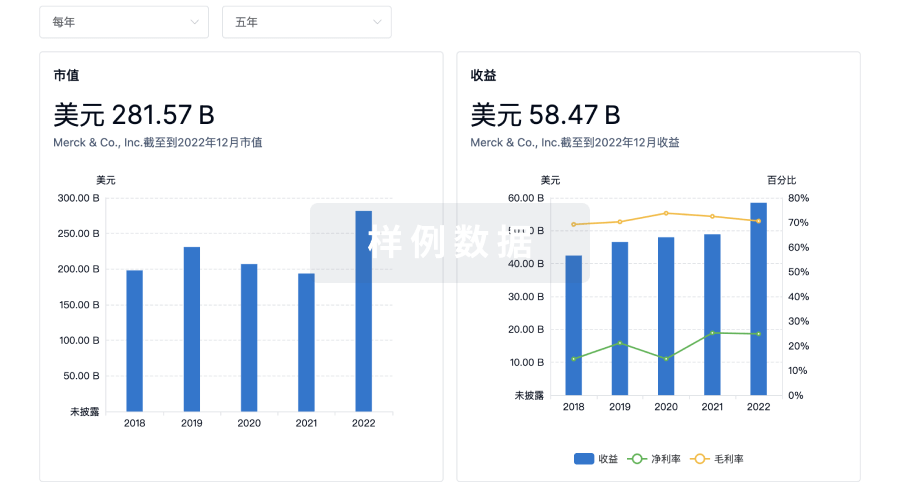
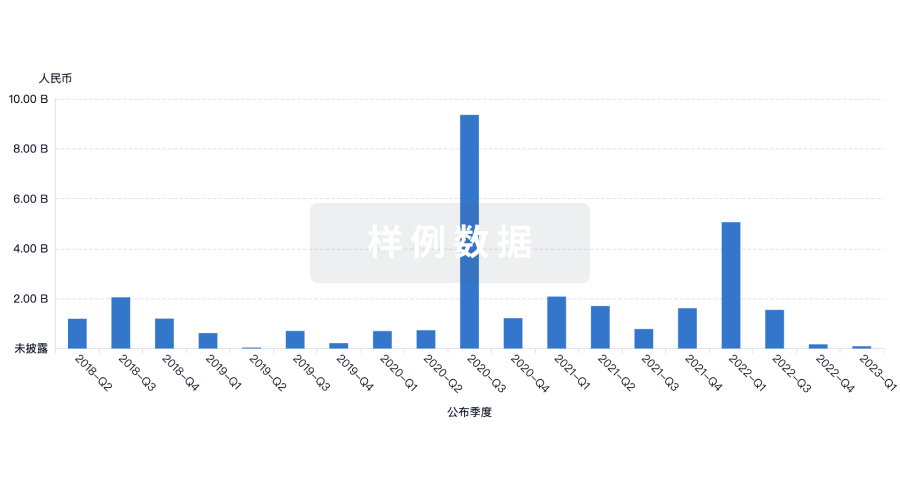
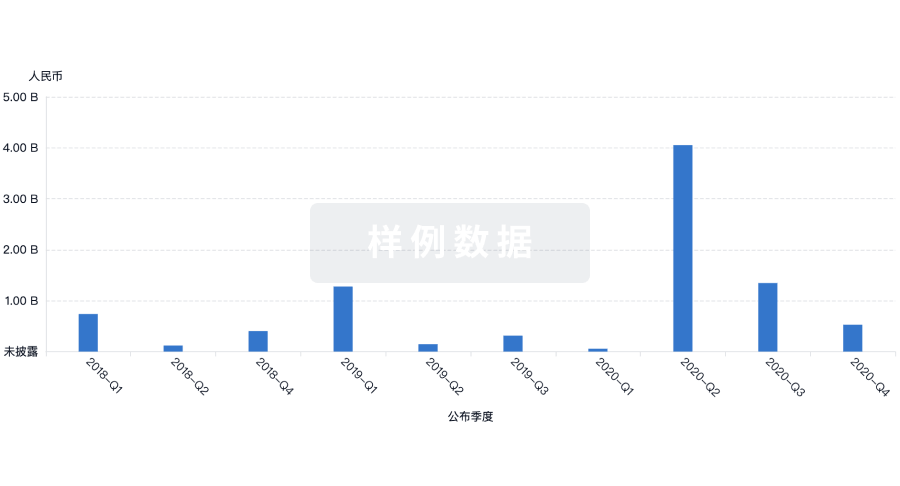
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用