更新于:2024-11-01
Japan National Hospital Organization
子公司|
Japan
子公司|
Japan
更新于:2024-11-01
概览
标签
感染
预防性疫苗

关联
1
项与 Japan National Hospital Organization 相关的药物靶点- |
作用机制- |
在研适应症 |
非在研适应症- |
最高研发阶段临床2期 |
首次获批国家/地区- |
首次获批日期- |
100 项与 Japan National Hospital Organization 相关的临床结果
登录后查看更多信息
0 项与 Japan National Hospital Organization 相关的专利(医药)
登录后查看更多信息
920
项与 Japan National Hospital Organization 相关的文献(医药)2023-11-02·Blood
Mixture Model to Predict the Cumulative Incidence of Relapses in Follicular Lymphoma : Need for Longer Follow-up or Alternative Outcomes
作者: Yokoyama, Hisayuki ; Cheung, Matthew C. ; Casanova, María ; Snauwaert, Sylvia ; Gyan, Emmanuel ; Fornecker, Luc-Matthieu ; Robu, Daniela ; Johnson, Nathalie A. ; Deconinck, Eric ; Van Den Neste, Eric ; Choudhary, Yuvraj ; Marjanovic, Zora ; Mace, Joseph Ronald ; Dorvaux, Veronique ; Yamamoto, Go ; Guidez, Stephanie ; Quick, Donald P. ; Foucher, Yohann ; Fabbro, Michel ; Morschhauser, Franck ; Terui, Yasuhito ; Glaisner, Sylvie
2023-04-01·Allergology International
Longitudinal changes in the prevalence of adult asthma: An epidemiological survey among Japanese salaried employees and their dependents using healthcare insurance claim from 1999 to 2019
Article
作者: Fukutomi, Yuma ; Watai, Kentaro ; Irie, Mari ; Tomita, Yasuhiro ; Fujisawa, Takao ; Nakamura, Yoichi ; Taniguchi, Masami ; Nagao, Mizuho ; Sekiya, Kiyoshi ; Shimoda, Terufumi ; Okada, Chiharu ; Kamide, Yosuke ; Hamada, Yuto ; Azekawa, Kazuhiro ; Nagayama, Kisako ; Nakatani, Eiji
2023-01-04·Journal of Occupational Health
Reliability and validity of the Japanese version of the Professional Fulfillment Index among healthcare professionals: A validation study
Article
作者: Ikeda, Miki ; Nishi, Daisuke ; Koido, Yuichi ; Sasaki, Natsu ; Kawashima, Yuzuru ; Miyamoto, Yuki ; Asaoka, Hiroki
100 项与 Japan National Hospital Organization 相关的药物交易
登录后查看更多信息
100 项与 Japan National Hospital Organization 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2024年11月05日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
临床2期
1
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或

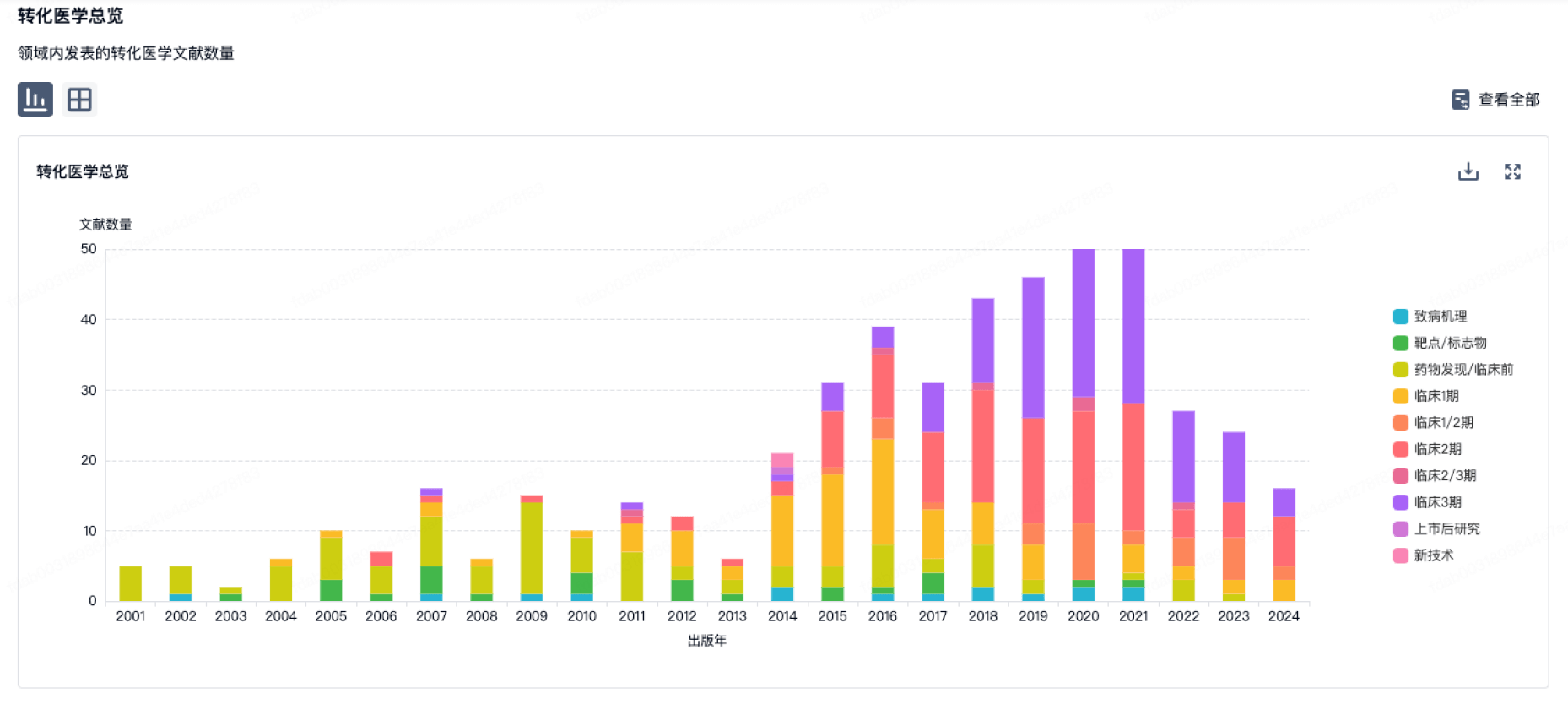
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
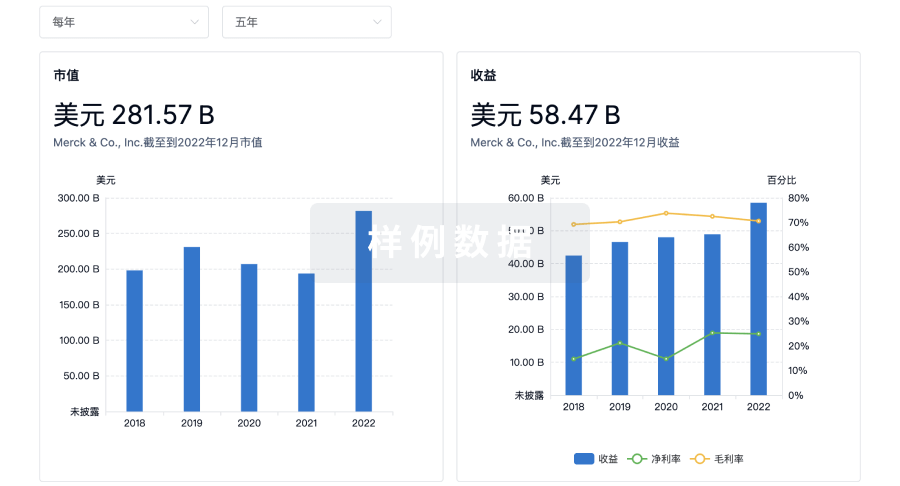
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或

融资
发掘融资趋势以验证和推进您的投资机会。
登录
或

标准版
¥16800
元/账号/年
新药情报库 | 省钱又好用!
立即使用
来和芽仔聊天吧
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用