预约演示
更新于:2025-08-27

Polaris Inc.
更新于:2025-08-27
概览
标签
血液及淋巴系统疾病
免疫系统疾病
酶
疾病领域得分
一眼洞穿机构专注的疾病领域

技术平台
公司药物应用最多的技术
靶点
公司最常开发的靶点
关联
靶点 |
作用机制 |
在研机构 |
原研机构 |
在研适应症 |
非在研适应症 |
最高研发阶段 |
首次获批国家/地区 |
首次获批日期 |
100 项与 Polaris Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2022-01-01LWT-FOOD SCIENCE AND TECHNOLOGY
Functional annotation unravels probiotic properties of a poultry isolate, Bacillus velezensis CGS1.1
作者: Ninad Pandit ; Christopher Dunlap ; Hareshkumar Keharia ; Jayraj Doshi ; Riteshri Soni
Probiotics are an eco-friendly and prospective substitute for antibiotic growth promoters.The present investigation aimed to dissect the probiotic attributes of a poultry isolate CGS1.1 by integrating genomics and phenotypic traits.The strain exhibited bile salt hydrolase activity and ∼73% survival in simulated gastrointestinal juices.It displayed notable aggregation, cell surface hydrophobicity, biofilm formation, and antimicrobial activity against gram-pos. and gram-neg. bacterial pathogens.Interestingly, the strain CGS1.1 completely inhibited the growth of E. coli and S. enterica after 24 h in liquid co-culture assay.The strain CGS1.1 effectively hydrolyzes starch, cellulose, pectin, tributyrin, casein, and phytate.The in silico genome anal. revealed its identity as Bacillus velezensis.Genome annotation revealed the presence of genes encoding the aforementioned probiotic properties.Furthermore, CGS1.1 was found to be non-hemolytic and sensitive to major classes of antibiotics.No potent virulent factor or toxin encoding genes could be predicted in CGS1.1 genome signifying its safety.The demonstrate the potential of CGS1.1 as a probiotic to promote chicken growth and control pathogens.
2021-12-15Cancer1区 · 医学
Assessment of pegylated arginine deiminase and modified FOLFOX6 in patients with advanced hepatocellular carcinoma: Results of an international, single‐arm, phase 2 study
1区 · 医学
Article
作者: Lee, Dae‐Won ; El Dika, Imane ; Huang, Wen‐Tsung ; Yang, Tsai‐Sheng ; Ryoo, Baek‐Yeol ; Ho, Ching‐Liang ; Qin, Shukui ; Chen, Yen‐Yang ; Sarker, Debashis ; Harding, James J. ; Meyer, Timothy ; O’Reilly, Eileen M. ; Cohen, Stacey A. ; Akce, Mehmet ; Tan, Benjamin ; Feng, Yin‐Hsun ; Johnston, Amanda ; Bomalaski, John S. ; Abou‐Alfa, Ghassan K. ; Lim, Ho Yeong ; Yen, Chia‐Jui
Background:
Arginine starvation depletes the micronutrients required for DNA synthesis and interferes with both thymidylate synthetase activity and DNA repair pathways in preclinical models of hepatocellular carcinoma (HCC). Pegylated arginine deiminase (ADI‐PEG 20), an arginine degrader, potentiates the cytotoxic activity of platinum and pyrimidine antimetabolites in HCC cellular and murine models.
Methods:
This was a global, multicenter, open‐label, single‐arm, phase 2 trial of ADI‐PEG 20 and modified 5‐fluorouracil, leucovorin, and oxaliplatin (mFOLFOX6) in patients who had HCC with Child‐Pugh A cirrhosis and disease progression on ≥2 prior lines of treatment. The primary objective was the objective response rate assessed according to Response Evaluation Criteria in Solid Tumors, version 1.1. Secondary objectives were to estimate progression‐free survival, overall survival, safety, and tolerability. Eligible patients were treated with mFOLFOX6 intravenously biweekly at standard doses and ADI‐PEG‐20 intramuscularly weekly at 36 mg/m2.
Results:
In total, 140 patients with advanced HCC were enrolled. The median patient age was 62 years (range, 30‐85 years), 83% of patients were male, 76% were of Asian race, 56% had hepatitis B viremia, 10% had hepatitis C viremia, 100% had received ≥2 prior lines of systemic therapy, and 39% had received ≥3 prior lines of systemic therapy. The objective response rate was 9.3% (95% confidence interval [CI], 5.0%‐15.4%), with a median response duration of 10.2 months (95% CI, 5.8 months to not reached). The median progression‐free survival was 3.8 months (95% CI, 1.8‐6.3 months), and the median overall survival was 14.5 months (95% CI, 13.6‐20.9 months). The most common grade ≥3 treatment‐related events were neutropenia (32.9%), white blood cell count decrease (20%), platelet count decrease (19.3%), and anemia (9.3%).
Conclusions:
Concurrent mFOLFOX6 plus ADI‐PEG 20 exhibited limited antitumor activity in patients with treatment‐refractory HCC. The study was terminated early, and no further evaluation of the combination will be pursued.
Lay Summary:
Arginine is an important nutrient for hepatocellular carcinoma (HCC).The depletion of arginine with pegylated arginine deiminase (ADI‐PEG 20), an arginine degrader, appeared to make chemotherapy (FOLFOX) work better in animal models of HCC and in patients with HCC on an early phase clinical trial.To formally test this hypothesis in the clinical setting, a large, global, phase 2 clinical trial was conducted of ADI‐PEG 20 and FOLFOX in the treatment of patients with refractory HCC.The study showed limited activity of ADI‐PEG 20 and FOLFOX in advanced HCC and was stopped early.
2021-10-01Journal of plastic, reconstructive & aesthetic surgery : JPRAS3区 · 医学
The chimeric medial sural artery perforator flap as the ideal for partial tongue reconstruction: A case series and technical refinements
3区 · 医学
Article
作者: Siti Radhziah Binte Sudirman ; Marcus J.M. Ng ; David Chang ; Adrian S.H. Ooi
BACKGROUND:
The medial sural artery perforator free flap (MSAP) has gained increasing popularity in head and neck reconstruction. Its slightly bulkier nature than the radial forearm flap, combined with negligible donor site morbidity, makes it an ideal candidate for the reconstruction of partial glossectomy defects. The ability to harvest the MSAP as a chimeric flap with a portion of the medial gastrocnemius muscle gives it greater flexibility in soft tissue reconstruction.
METHODS:
A retrospective study of patients with partial glossectomy defects reconstructed using the MSAP by a single surgeon was performed. Perioperative data, donor and recipient site characteristics, complications, and outcomes were analyzed. A video is included to show technical points for the harvest of the flap.
RESULTS:
A total of 10 patients were included. The average age was 59.1 years, with a mean of 43.5% of the tongue resected. All flaps survived, with no major complications. At follow-up, the patients had regained an average of 86.5% of original speech, with none requiring NG feeding. The average MSAP skin flap thickness was 7.8 mm, with 6 flaps being harvested as chimeric fasciocutaneous muscle flaps. Five flaps incorporated 2 perforators. Two case examples are presented.
CONCLUSION:
The chimeric MSAP perforator allows for more robust partial glossectomy reconstruction with improved postoperative functional outcomes. It should be considered as the workhorse flap for partial tongue reconstruction.
2025-04-27
2025-03-23
疫苗临床研究
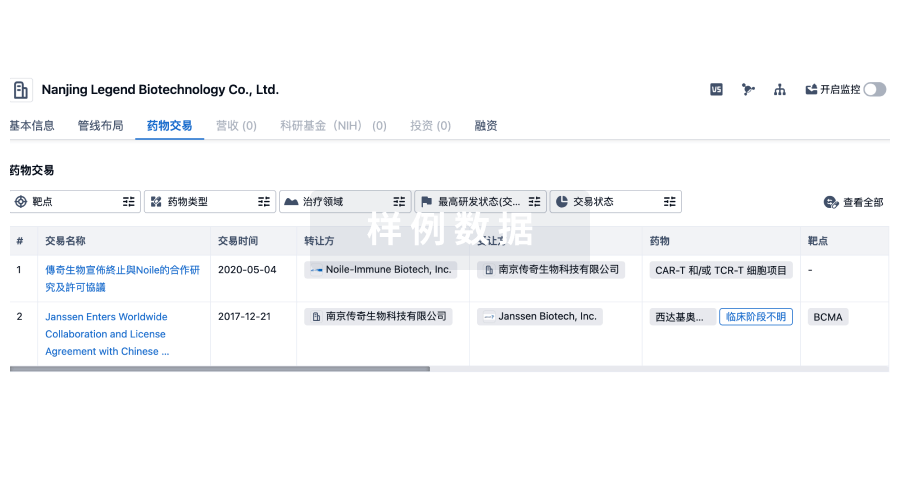
100 项与 Polaris Inc. 相关的药物交易
登录后查看更多信息
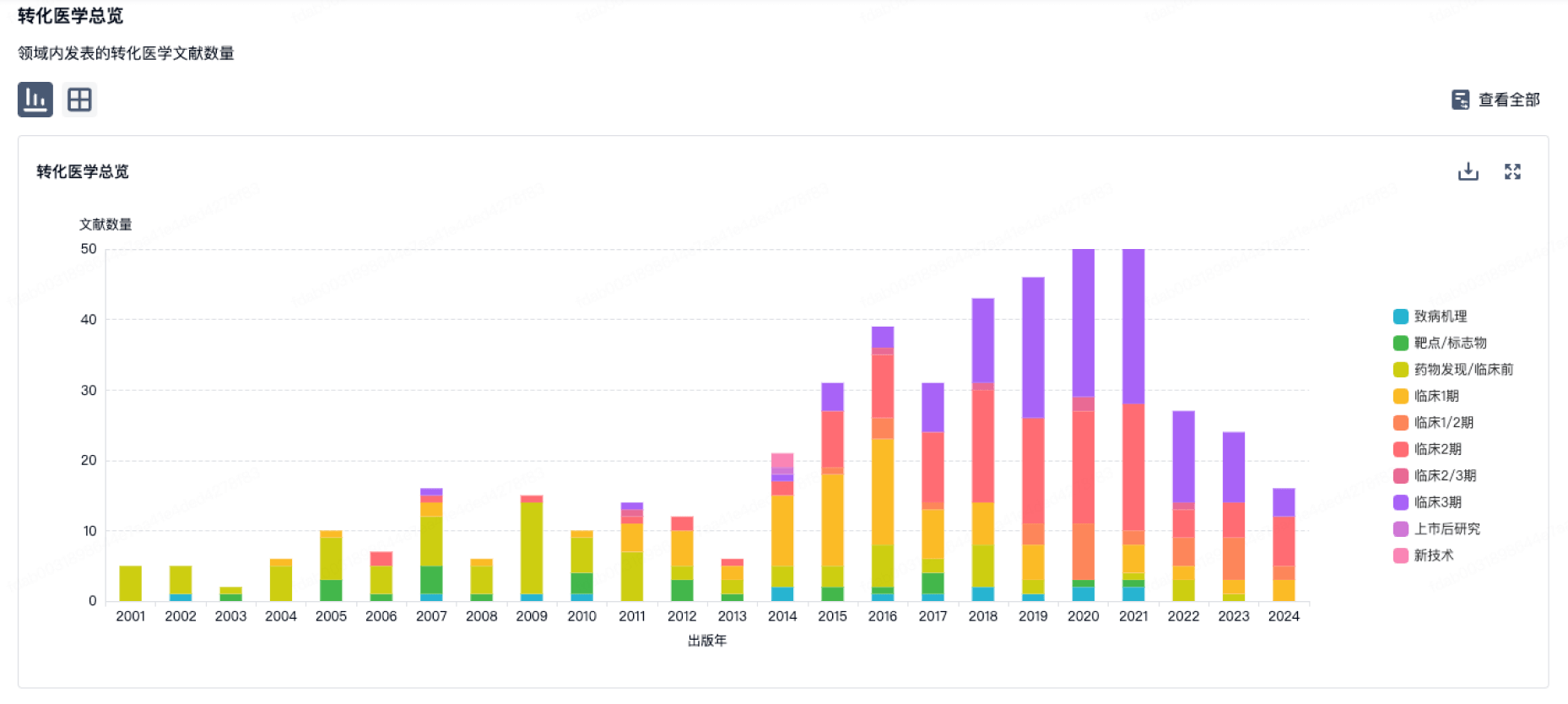
100 项与 Polaris Inc. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年08月30日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
临床2期
1
登录后查看更多信息
当前项目
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
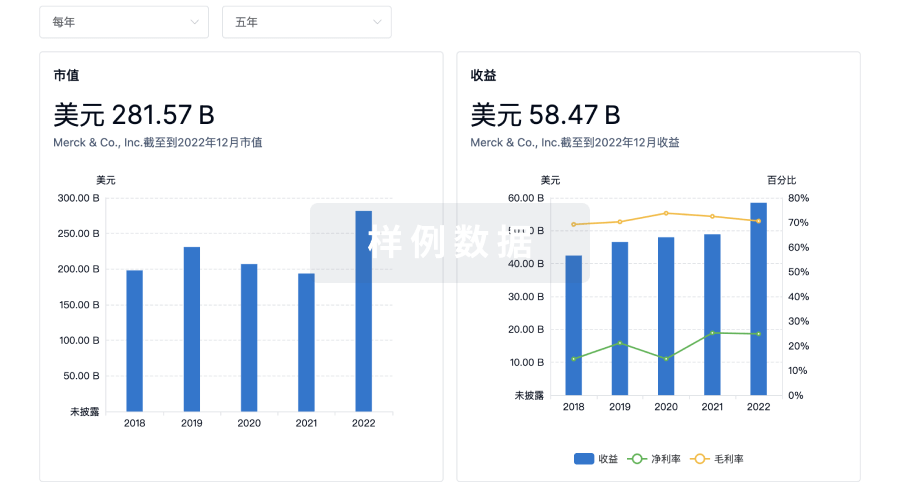
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用