更新于:2024-12-19

Callen-Lorde Community Health Center
更新于:2024-12-19
概览
关联
Testosterone Effects on Sexual Health in Transgender Men: Feasibility Study of an Oral Intervention
MyPEEPS (Male Youth Pursuing Empowerment, Education, and Prevention Around Sexuality) Mobile for Young Transgender Men

Transgender Cohort Study of Gender Affirmation and HIV-related Health
100 项与 Callen-Lorde Community Health Center 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2024-12-01Journal of Pediatric and Adolescent Gynecology
NASPAG Clinical Opinion: The Care of Transgender and Gender Nonbinary Adolescents and Young Adults
Article
作者: Jarin, Jason ; Trotman, Gylynthia ; Krempasky, Chance ; Belkind, Uri ; Grimstad, Frances ; Cizek, Stephanie
Transgender and gender nonbinary (TGNB) adolescents and young adults (AYA) may present to clinicians with reproductive health expertise for the spectrum of gynecologic, sexual, and reproductive care. As such, clinicians should be knowledgeable in the many facets of gender-affirming care. This clinical opinion reviews language associated with gender diversity and gender-affirming care; current clinical, social, and political barriers faced by TGNB AYA; and the creation of welcoming and inclusive clinical spaces for TGNB AYA. It discusses social, medical, and surgical affirmation processes, and focuses on gynecologic care topics which may arise in the care of TGNB AYA, including those who undergo medical or surgical therapies. This includes menstrual suppression, breakthrough bleeding on testosterone, sexual health, fertility, and the pelvic care of individuals following gender affirming vulvovaginoplasty.
2024-10-01AIDS AND BEHAVIOR
To Improve Motivational Barriers to Retention in High Resolution Anoscopy, Patients and Providers Recommend Social and Environmental Changes: A Sequential Explanatory Mixed-Methods Pilot Study in a Federally Qualified Health Center
Article
作者: Rael, Christine Tagliaferri ; Hou, Baichun ; DeWitt, Will ; Tan, Mei ; Sandfort, Theodorus G M ; Giguere, Rebecca ; Kutner, Bryan A ; Radix, Asa
Abstract:
Loss to follow-up (LTFU) in high-resolution anoscopy (HRA) programs jeopardizes the procedure’s potential to help prevent anal cancer. We explored quality improvement factors to understand how to address this LTFU. Using the transtheoretical COM-B Model (Capability, Opportunity, Motivation, and Behavior) and a sequential explanatory mixed-methods design, we surveyed and interviewed 13 patients who remained engaged in HIV care but who delayed their HRA monitoring or treatment visits in the same community clinic, and 6 HRA clinicians and medical assistants. Analyses involved descriptive statistics and rapid qualitative analysis. Patients were racially, ethnically, and economically representative of the LTFU population, and were generally experienced with HRA (Mean HRA visits = 4.6, SD = 2.8, mdn = 3). Providers were experienced clinicians and medical assistants (Mean years providing HRA = 6.0, SD = 2.2). Analyses revealed two primary, related barriers: (A) motivational barriers such as physical pain, discomfort, embarrassment, and anxiety; which were largely borne from (B) opportunity barriers such as difficulties with scheduling, inconsistent after-care (particularly for pain and discomfort), anxiety-inducing exam rooms and equipment, and internalized and anticipated stigma. Capability barriers, such as limited health literacy about HRA, were less common and, like motivational barriers, linked to opportunity barriers. Participants recommended potential facilitators, including easier scheduling, standardization of pain management and after-care services, and examination room modifications to reduce anxiety. To retain HRA patients in community settings, interventions should address social and physical opportunity barriers that strongly determine motivational and capability barriers. Improving convenience, standardizing pain management, and introducing stigma interventions specific to HRA, could alleviate both motivational and capability barriers.
2024-10-01AMERICAN JOURNAL OF PREVENTIVE MEDICINE
Hormones, Stress, and Heart Disease in Transgender Women with HIV in LITE Plus
Article
作者: Juster, Robert-Paul ; Rich, Ashleigh ; Streed, Carl G. ; Reisner, Sari L. ; Perreira, Krista M ; Ehrig, Molly ; Cannon, Christopher ; Cortina, Christopher ; DuBois, L Zachary ; Mayer, Kenneth H. ; Poteat, Tonia C ; Wirtz, Andrea L ; Poteat, Tonia C. ; Malone, Jowanna ; Toribio, Mabel ; Radix, Asa E ; Malik, Mannat ; DuBois, L. Zachary ; Mayer, Kenneth H ; Ahmadi, Hedyeh ; Radix, Asa E. ; Streed, Carl G ; Perreira, Krista M. ; Wirtz, Andrea L. ; Reisner, Sari L
INTRODUCTION:
Cardiovascular disease (CVD) is a leading cause of death among transgender women and people with HIV. Exogenous estrogen and psychosocial stressors are known risk factors for CVD. Yet, few studies have used biomarkers to examine the role of stress in CVD risk among transgender women with HIV (TWHIV). This analysis examined whether stress moderates relationships between gender-affirming hormone therapy (GAHT) duration and CVD risk among TWHIV.
METHODS:
This cross-sectional analysis of baseline data from an observational cohort of 108 Black and Latina TWHIV in Boston, New York, and Washington, DC, enrolled December 2020 to June 2022, measured sociodemographics, medical diagnoses, medications, smoking history, and perceived stress via interviewer-administered surveys. Physiological stress was measured with 14 biomarkers to calculate allostatic load indices (ALI). Forty participants provided saliva samples used to calculate cortisol awakening response and cortisol daily decline. The 2018 American College of Cardiology Revised Pooled Cohort Equation estimated 10-year CVD risk. Data were analyzed in 2024.
RESULTS:
GAHT duration was positively associated with CVD risk scores in bivariate regression. In multivariable linear regression models (adjusting for age, income, education), only age and ALI remained significantly associated with CVD risk scores (β 1.13, CI: 1.05, 1.21). No stress measure significantly interacted with GAHT duration to affect CVD risk scores. In visual plots, GAHT duration increased CVD risk scores only for TWHIV experiencing the highest ALI.
CONCLUSIONS:
Stress plays an important role in CVD in TWHIV. More research is needed on non-GAHT factors, which influence CVD health among transgender women.
100 项与 Callen-Lorde Community Health Center 相关的药物交易
登录后查看更多信息
100 项与 Callen-Lorde Community Health Center 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2024年12月22日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
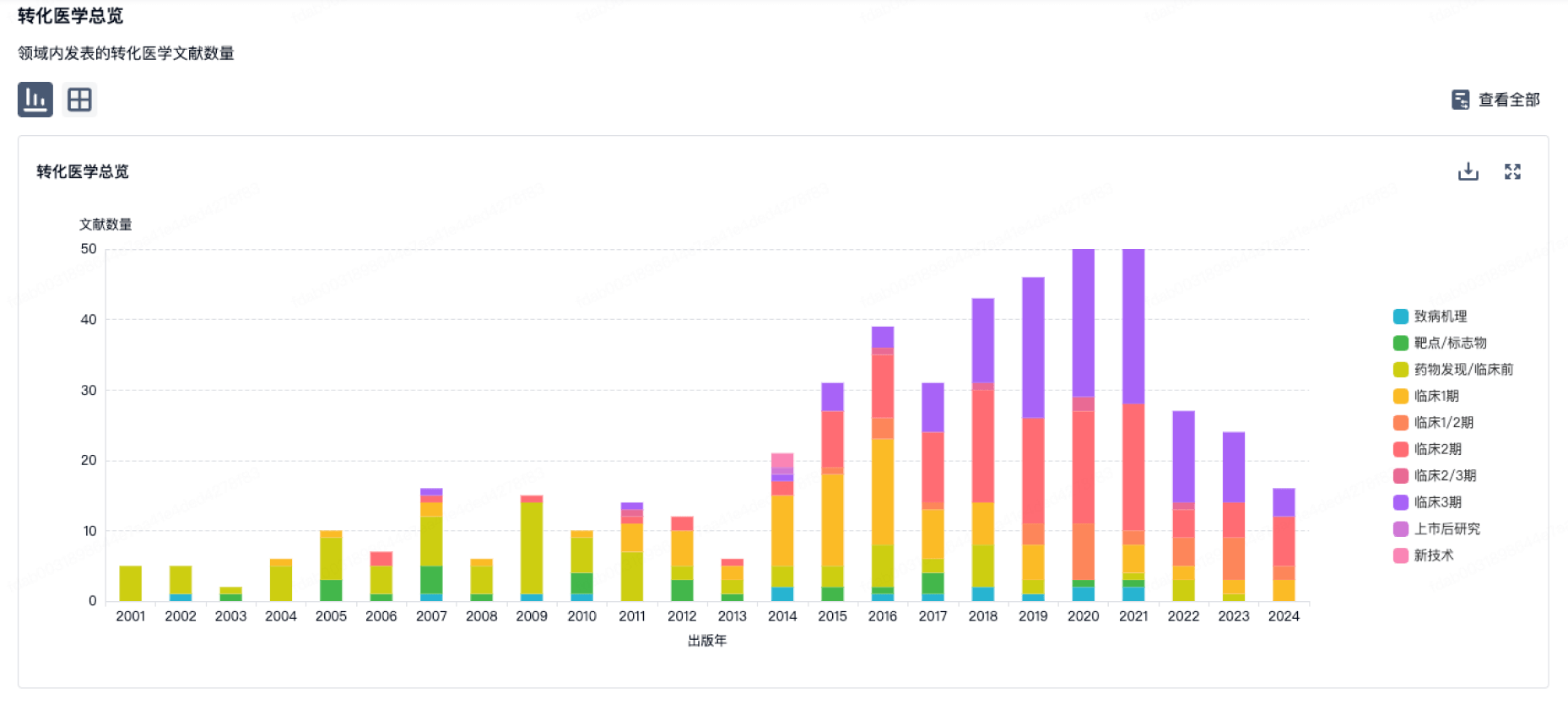
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
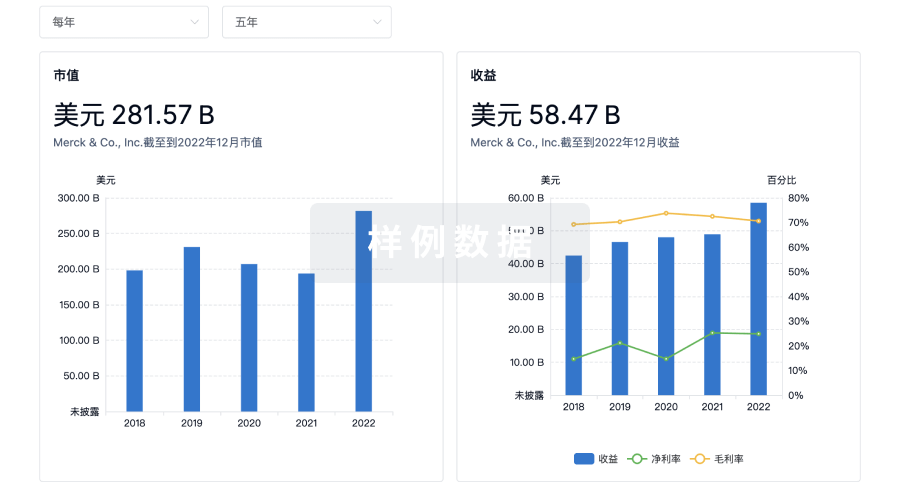
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
来和芽仔聊天吧
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用