预约演示
更新于:2025-05-07

Texas Scottish Rite Hospital for Children
更新于:2025-05-07
概览
关联
NCT06559215
Prospective Evaluation of Post-operative Pain Management Using Exparel in the Pediatric Population
NCT06559137
Prospective Evaluation of Post-operative Pain Management Using Peripheral Nerve Blocks in the Pediatric Population
NCT06048419
Acceptability and Efficacy of GO MOVE: A Mobile Health Technology for Youth With Unilateral Cerebral Palsy
100 项与 Texas Scottish Rite Hospital for Children 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-05-12Brain Injury
Endophenotype presentation of athletes with concussion contingent on sex and time since injury
Article
作者: Cullum, C Munro ; Beitchman, Joshua A ; Chung, Jane S ; Stokes, Mathew ; Didehbani, Nyaz ; Miller, Shane M ; Hynan, Linda S ; Jones, Jacob C
2025-03-01Spine Deformity
Spine deformity surgery in patients with Beals syndrome can be effectively performed but does risk revision surgery
Article
作者: Datcu, Anne-Marie ; Thornberg, David ; Booth, Anna ; Sucato, Daniel J ; Sucato, Daniel J.
2025-03-01Clinical Orthopaedics & Related Research
Clinical Faceoff: The Role of Elective Bilateral Lower Limb Lengthening for Gaining Height
Article
作者: Birch, John ; Sabharwal, Sanjeev ; Paley, Dror
2024-03-11
100 项与 Texas Scottish Rite Hospital for Children 相关的药物交易
登录后查看更多信息
100 项与 Texas Scottish Rite Hospital for Children 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年07月14日管线快照
无数据报导
登录后保持更新
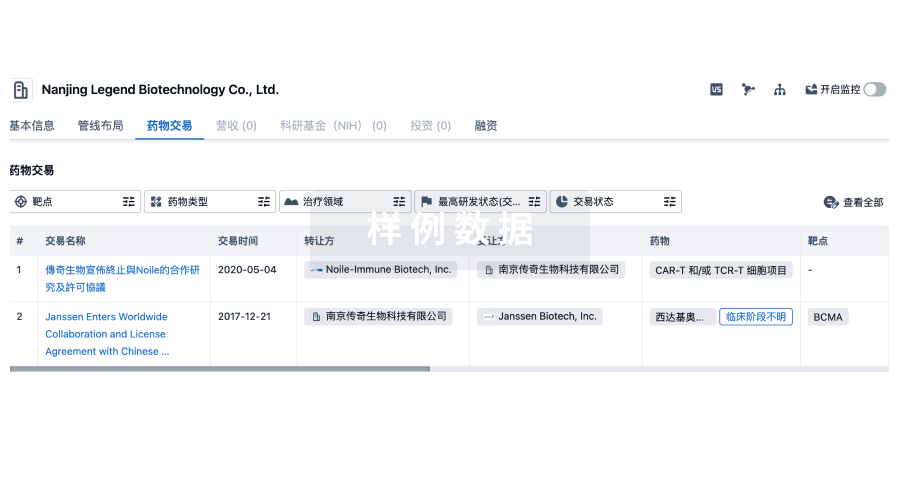
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
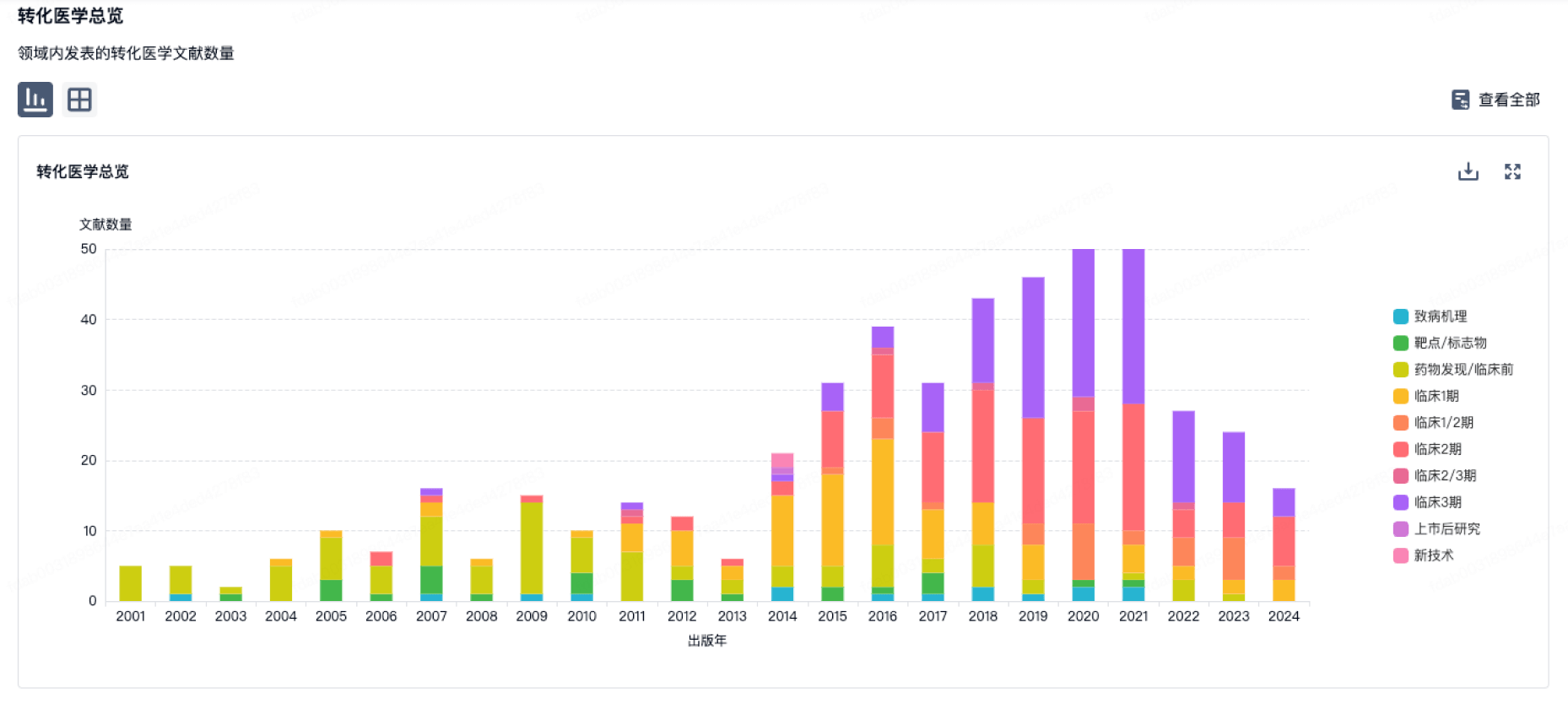
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
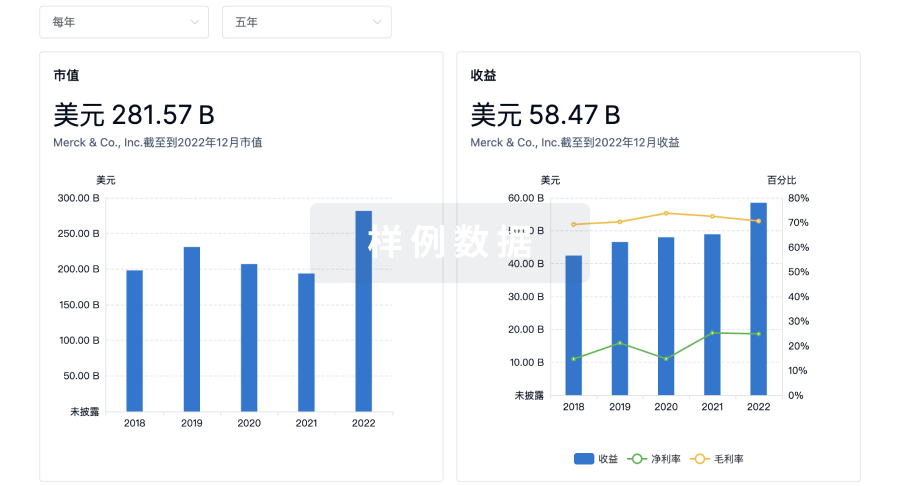
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用