预约演示
更新于:2025-05-07
Centre integre universitaire de sante & de services sociaux
更新于:2025-05-07
概览
关联
2
项与 Centre integre universitaire de sante & de services sociaux 相关的临床试验NCT06620393
Effects of Dexmedetomidine on Agitation in Critically Ill TBI Patients (DEX-TBI)
Agitation is a frequent complication following traumatic braing injury in patients admitted to the intensive care unit. This agitation frequently results in the liberal use of rescue drugs such as antipsychotics, sedatives and opiates, which in turn may delay rehabilitation, liberation from mechanical ventilation and emergence from posttraumatic amnesia. Dexmedetomidine may be a better agent given it's light sedative properties. The main objective is to assess the feasibility of conducting a multicenter randomized controlled trial of dexmedetomidine following TBI in the ICU.
开始日期2024-10-01 |
ISRCTN93896690
Efficacy of the Mirror Effect rehabilitation in acute Bell’s Palsy: a pilot study
开始日期2017-02-27 |
100 项与 Centre integre universitaire de sante & de services sociaux 相关的临床结果
登录后查看更多信息
0 项与 Centre integre universitaire de sante & de services sociaux 相关的专利(医药)
登录后查看更多信息
5
项与 Centre integre universitaire de sante & de services sociaux 相关的文献(医药)2025-02-10·Journal of Clinical Oncology
Impact of testosterone recovery after androgen deprivation therapy on overall survival in patients with high-risk prostate cancer: Long-term data from a phase III trial.
作者: Vincent, Francois ; Bettahar, Redouane ; Souhami, Luis ; Bahoric, Boris ; Martin, Andre-Guy ; Vass, Sylvie ; Archambault, Robert ; Nabid, Abdenour ; Bahary, Jean-Paul ; Carrier, Nathalie ; Vavassis, Peter ; Duclos, Marie
2024-06-01·Journal of Clinical Oncology
Evaluation of recurrence rate in Canadian patients with stage II/III HR+/HER2- early breast cancer in the real-world setting.
作者: Mackay, Helen ; Gambaro, Karen ; Abdelsalam, Mahmoud ; Boudreau, Dominique ; Basik, Mark ; Patel, Chandni ; St-Hilaire, Eve ; Guillemette, Stephanie ; Hassan, Saima Noor ; Saad, Fred ; Caron, Marc-Andre ; Leite, Ricardo ; Vincent, Francois ; Batist, Gerald ; Marques, Maud
2024-06-01·Journal of Clinical Oncology
Quality of life and testosterone recovery after androgen deprivation therapy in patients with high-risk prostate cancer: Long-term data from a phase III trial.
作者: Vincent, Francois ; Bettahar, Redouane ; Bahoric, Boris ; Vass, Sylvie ; Archambault, Robert ; Martin, André-Guy ; Nabid, Abdenour ; Souhami, Luis ; Carrier, Nathalie ; Vavassis, Peter ; Bahary, Jean-Paul
100 项与 Centre integre universitaire de sante & de services sociaux 相关的药物交易
登录后查看更多信息
100 项与 Centre integre universitaire de sante & de services sociaux 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年07月22日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
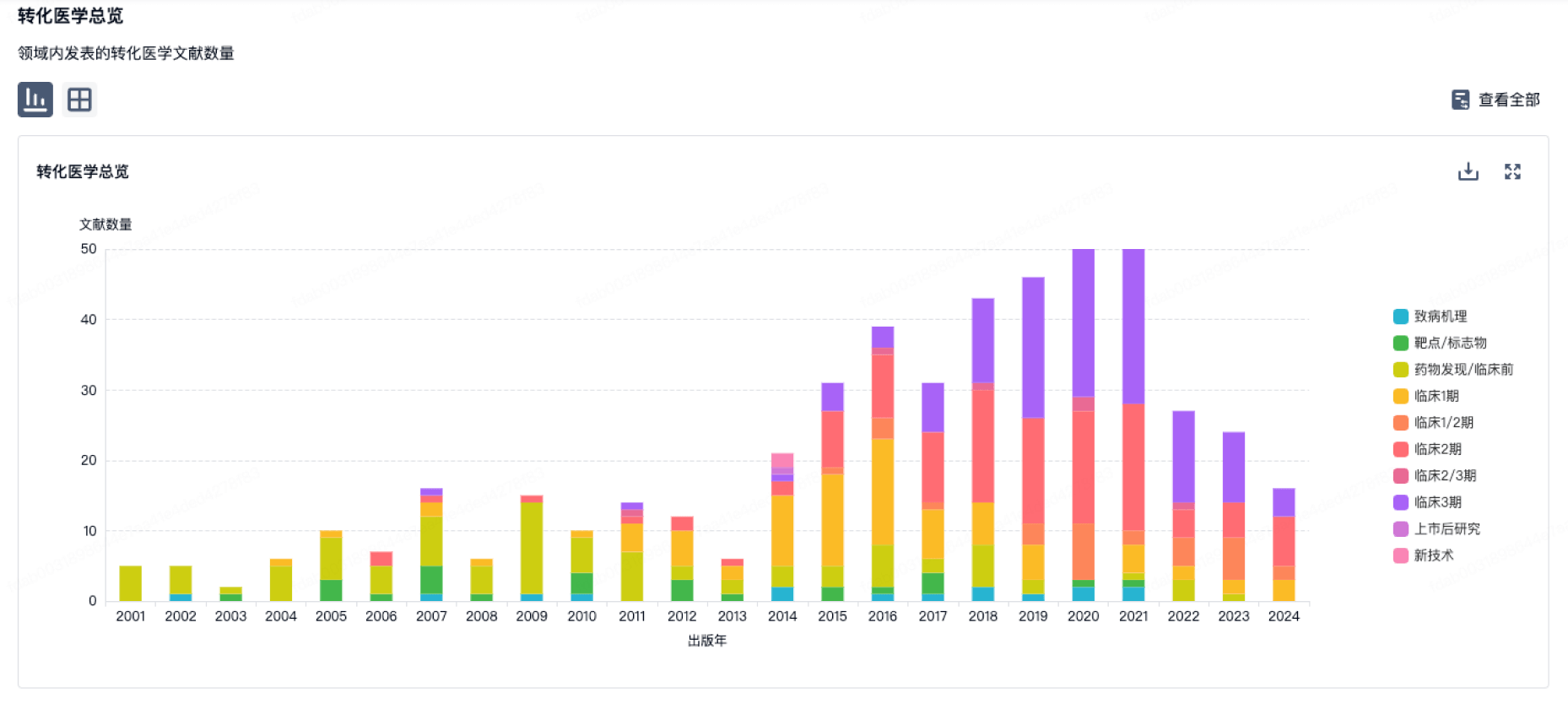
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
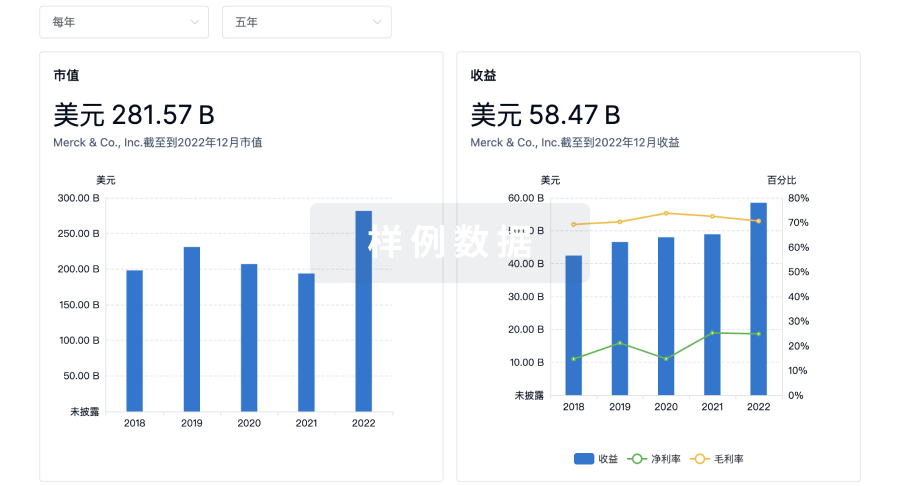
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用