更新于:2024-06-20
Asthma therapeutics(Regenecore)
更新于:2024-06-20
概要
基本信息
原研机构 |
在研机构- |
非在研机构 |
最高研发阶段未知 |
首次获批日期- |
最高研发阶段(中国)未知 |
特殊审评- |
关联
100 项与 Asthma therapeutics(Regenecore) 相关的临床结果
登录后查看更多信息
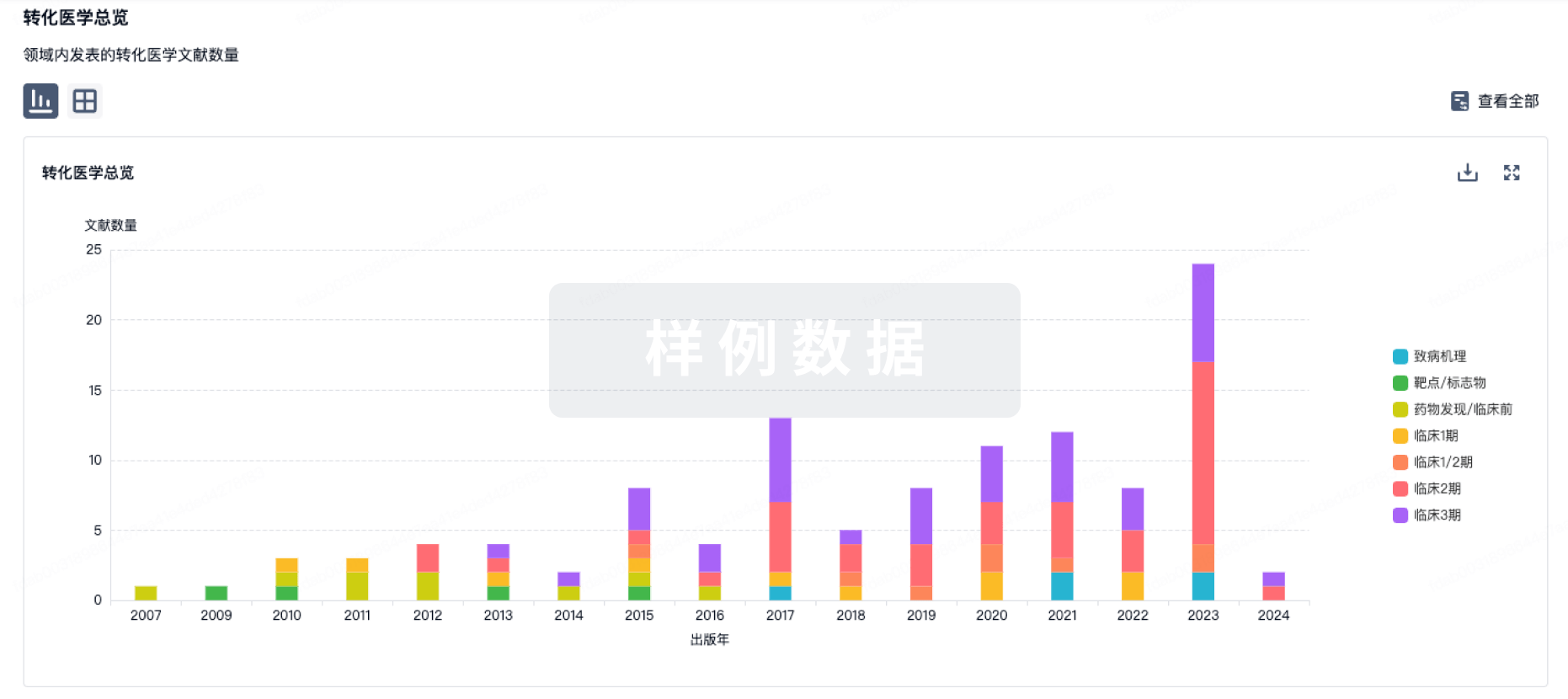
100 项与 Asthma therapeutics(Regenecore) 相关的转化医学
登录后查看更多信息
100 项与 Asthma therapeutics(Regenecore) 相关的专利(医药)
登录后查看更多信息
12
项与 Asthma therapeutics(Regenecore) 相关的文献(医药)2021-12-01·Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology2区 · 医学
Asthma biologics
2区 · 医学
Article
作者: Sandhya Khurana ; Steve Georas ; Farrukh Abbas ; Xueya Cai
BACKGROUND:
Confirmation of effectiveness of asthma biologics in the real world is desirable because patient characteristics and experiences may differ from those included in randomized controlled trials.
OBJECTIVE:
To evaluate real-world effectiveness of asthma biologics and identify predictors of response.
METHODS:
We performed a retrospective study in patients with severe asthma receiving biologics. The primary outcome was change in clinically significant exacerbations at 12 months after starting biologic therapy, compared with 12 months before. Secondary outcomes were change in severe exacerbations, maintenance oral corticosteroid (OCS) dose, prebronchodilator forced expiratory volume in 1 second (FEV1), and asthma control test scores. Subgroup analyses were performed for subjects who were biologic naive or not. A stepwise logistic regression model was performed to compare responders to nonresponders.
RESULTS:
A total of 112 patients were included. Biologic therapy was associated with a 59% reduction in clinically significant exacerbations (P < .001), 65% reduction in severe exacerbations (P < .001), and 54% reduction in maintenance OCS dose (P = .001) in the 12 months after starting therapy. Biologics also resulted in improvement in prebronchodilator FEV1 (P = .002) and Asthma Control Test score (P < .001). Subjects who were previously on another biologic also experienced significant improvements in exacerbation frequency, maintenance OCS dose, and asthma control. Responders were more likely to be nonsmokers and have higher baseline FEV1, gastroesophageal reflux disease, and eosinophil counts greater than 500 cells/μL.
CONCLUSION:
In a real-world setting, biologic therapy in asthma is effective in improving exacerbations, asthma control, and lung function. Patients who have a suboptimal response to 1 biologic can still benefit from treatment with a different biologic.
2021-03-01·The journal of allergy and clinical immunology. In practice1区 · 医学
The Relationship of Asthma Biologics to Remission for Asthma
1区 · 医学
Article
作者: Andrew Menzies-Gow ; Stanley J. Szefler ; William W. Busse
Asthma treatments have evolved from bronchodilators to interventions directed toward the regulation of airway inflammation. From these advances has come greater disease control and reduced morbidity. The addition of biologics directed toward specific pathways of inflammation has advanced the efficacy of asthma control. With these treatment advances, a renewed interest in achieving a remission in asthma has arisen. Although asthma remission has been considered to reflect a "cure," new evaluations of this concept have proposed criteria for remission while on treatment. These criteria reflect a high level of disease control including absence of symptoms, optimization and stabilization of lung function, and absence of the use of systemic corticosteroids and have been proposed to indicate a remission of disease activity. Given the added efficacy found with biologics in asthma treatment for patients with moderate to severe disease, the question has arisen as to whether the use of biologics meets criteria for remission and may this change a component of underlying disease and risks. Biologics are highly effective in reducing exacerbations, diminishing symptoms, and improving lung function in well-defined asthma populations. At present, however, biologics achieve some, but in most cases not all criteria for a remission on treatment. However, the concept of promoting treatment efforts to achieve disease remission in asthma is important, potentially achievable, and merits consideration for future guideline-directed care approaches.
2021-03-01·Chest
Adherence to Asthma Biologics
Article
作者: Nilay D. Shah ; Regina W. Lam ; Molly M. Jeffery ; Jonathan W. Inselman ; Matthew A. Rank ; Jacob T. Maddux
BACKGROUND:
Little is known about adherence to asthma biologics.
RESEARCH QUESTION:
Is adherence to inhaled corticosteroid (ICS) associated with subsequent asthma biologic adherence?
STUDY DESIGN AND METHODS:
We analyzed individuals with asthma who started asthma biologics in the OptumLab Data Warehouse and used that data until October 2019. We calculated proportion days covered (PDC) for ICS ± long-acting β-agonists in the 6 months before and after asthma biologics were started and asthma biologic PDC for the first 6 months of use. We performed a multivariable analysis to identify factors associated with asthma biologic PDC ≥0.75, ICS PDC ≥0.75 during the 6-month period after asthma biologic were started, and achievement of a ≥50% reduction in asthma exacerbations during the first 6 months of asthma biologic use.
RESULTS:
We identified 5,319 people who started asthma biologics. The mean PDC for asthma biologics was 0.76 (95% CI, 0.75-0.77) in the first 6 months after starting, higher than the mean PDCs for ICS in the 6 months before (0.44 [95% CI, 0.43-0.45]) and after (0.40 [95% CI, 0.39-0.40]) starting the asthma biologic. PDC ≥0.75 for ICS 6 months before index biologic use is associated with PDC for asthma biologics ≥0.75 (OR, 1.25; 95% CI, 1.10-1.43) and for ICS during the first 6 months of biologic use (OR, 9.93; 95% CI, 8.55-11.53). Neither ICS PDC ≥0.75 (OR, 0.92; 95% CI, 0.74-1.14) nor asthma biologic PDC ≥0.75 (OR, 1.15; 95% CI, 0.97-1.36) is associated with a statistically significant reduction in asthma exacerbations during the first 6 months of asthma biologic use among people with any exacerbation in the 6 months before first use.
INTERPRETATION:
Adherence to asthma biologic is higher than to ICS and is associated with different factors.
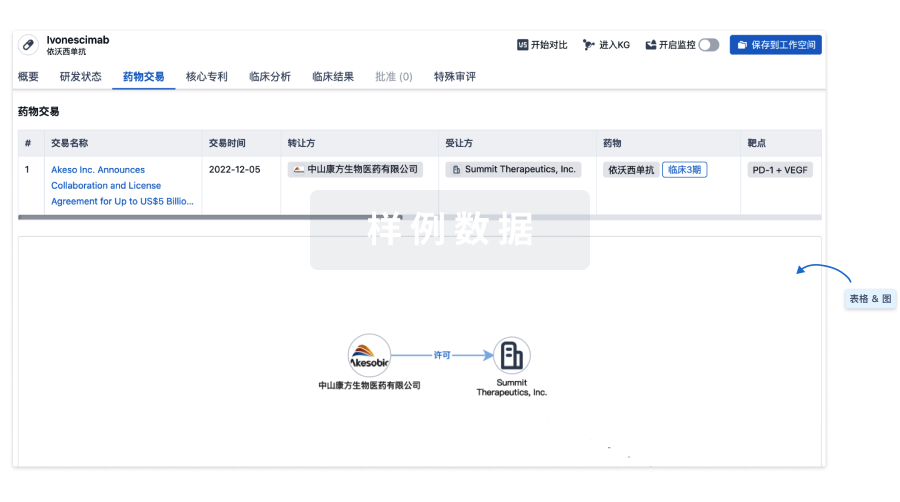
100 项与 Asthma therapeutics(Regenecore) 相关的药物交易
登录后查看更多信息
研发状态
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
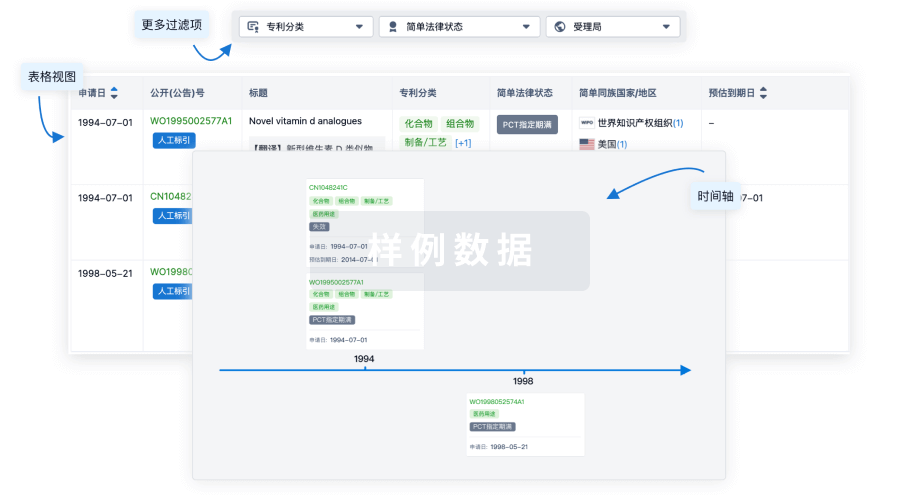
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
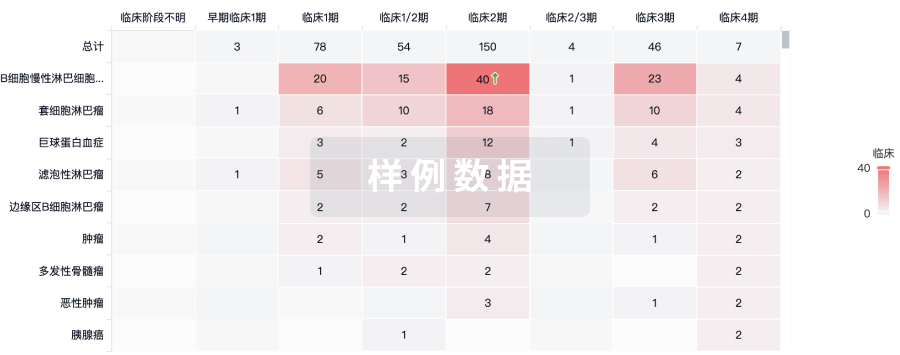
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

标准版
¥16800
元/账号/年
新药情报库 | 省钱又好用!
立即使用
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用