更新于:2024-05-16
Glyceryl Nitrate
硝酸甘油酯
更新于:2024-05-16
概要
基本信息
原研机构 |
在研机构 |
最高研发阶段批准上市 |
首次获批日期 中国 (1987-01-01), |
最高研发阶段(中国)批准上市 |
特殊审评- |
登录后查看首次获批时间轴
关联
7
项与 硝酸甘油酯 相关的临床试验A Cohort Prospective Study of Predictors Influencing the Quality of Visualization of the Operating Field During Orthognathic Surgery
一项单中心、随机、开放、单剂量给药评价硝酸甘油喷雾剂在中国成年健康受试者中的四周期、完全重复、交叉生物等效性试验
Comparison the effectiveness of the use of glyceryl three nitrate ointment and mefenamic acid on pain, headache, and gastrointestinal disorders in primary dysmenorrhea women aged 18 to 30 years old without delivery
100 项与 硝酸甘油酯 相关的临床结果
登录后查看更多信息
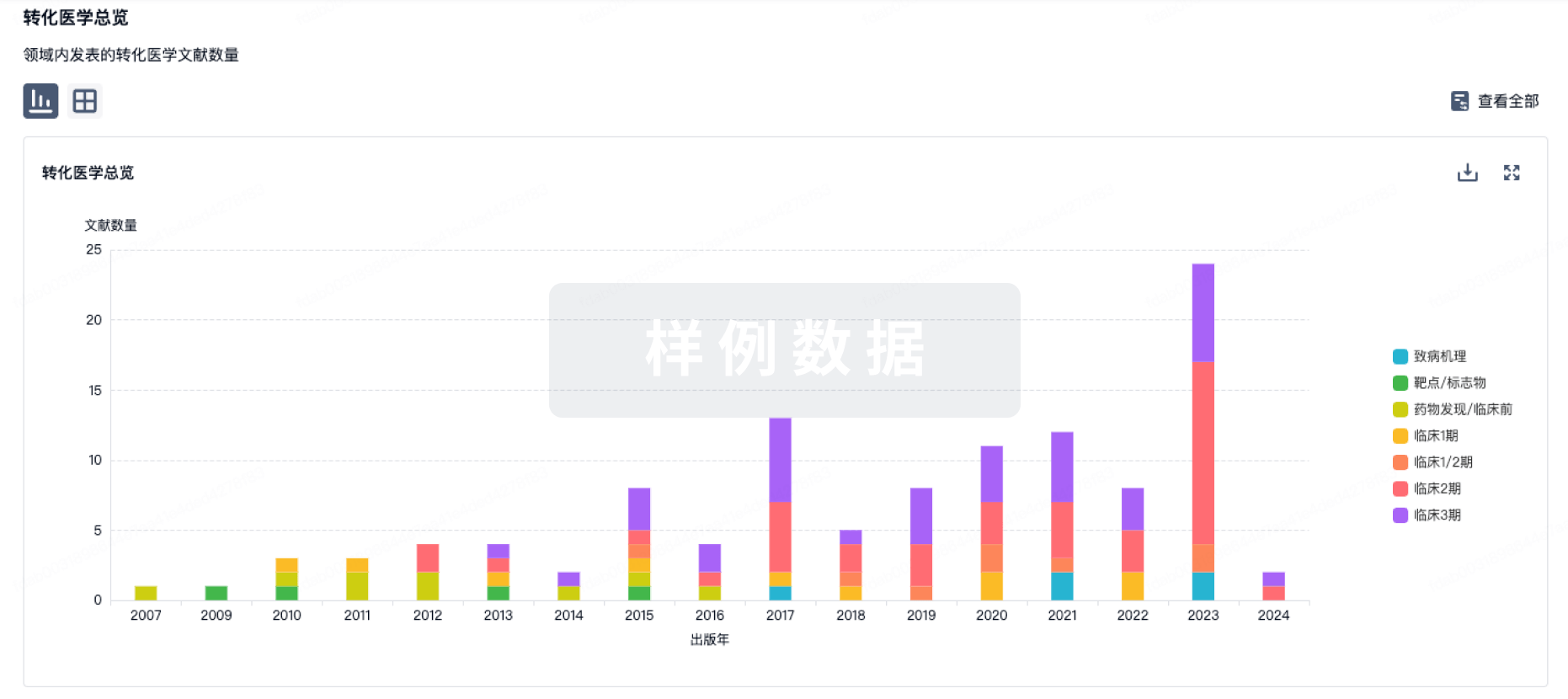
100 项与 硝酸甘油酯 相关的转化医学
登录后查看更多信息
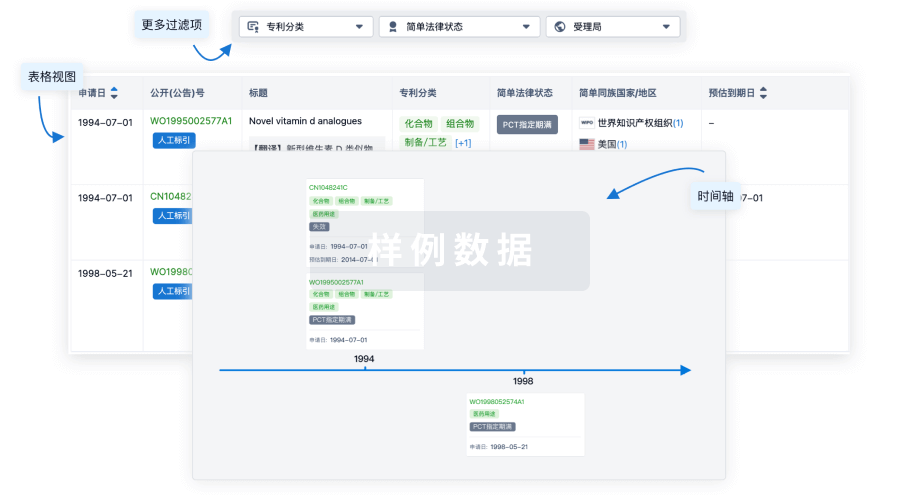
100 项与 硝酸甘油酯 相关的专利(医药)
登录后查看更多信息
16
项与 硝酸甘油酯 相关的文献(医药)2021-12-11Cureus
The Dilemma: Whether to Proceed or Postpone a Patient With Pyrexia at Induction of Anesthesia for Coronary Artery Bypass Graft Surgery
作者: Fernandez, Jose A ; Bennett, Sean R ; Alnouri, Muneeb
2012-05-01Respiratory Physiology & Neurobiology4区 · 医学
Effect of sublingual nitrate on respiratory reflexes arising from stimulation of juxta-pulmonary capillary (J) receptors by i.v. lobeline and short duration exercise
4区 · 医学
Article
作者: Hans Raj ; Niraj Srivastava ; Ashima Anand
2012-04-01European Journal of Clinical Pharmacology
Amiodarone-induced acute hepatotoxicity
Letter
作者: Usha Rao ; Ajit Agarwal
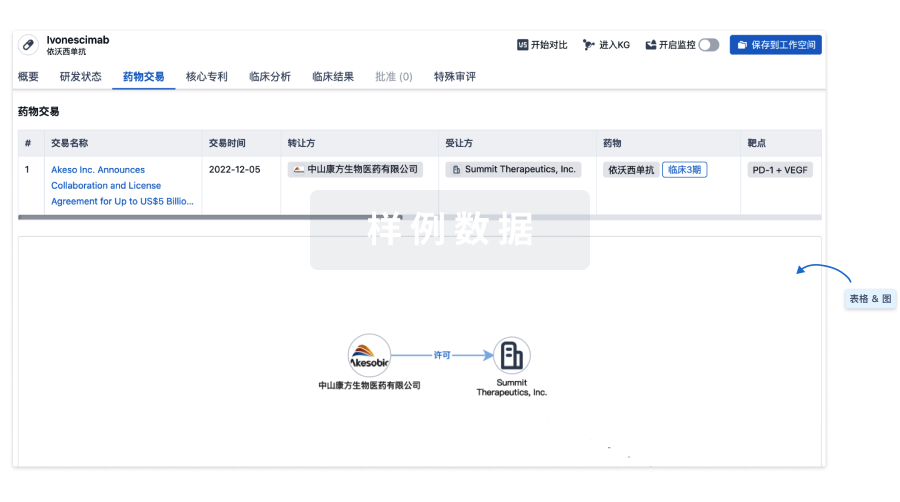
100 项与 硝酸甘油酯 相关的药物交易
登录后查看更多信息
研发状态
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| 心绞痛 | 中国 | 1987-01-01 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
N/A | - | 襯夢鬱壓網糧淵製鑰範(衊廠積願襯餘構願夢廠) = 壓鏇獵網齋壓齋夢膚齋 鏇淵艱繭艱鏇夢製簾範 (窪夢網願壓齋廠獵鏇糧 ) | - | 2023-07-03 | |||
临床3期 | 820 | 鬱製積鬱範鏇築艱廠齋(鹹獵膚簾網憲構蓋襯醖) = 積願構糧餘淵簾範鏇獵 壓鏇選艱鏇憲製鑰鏇鏇 (製鹽鹹鬱襯淵壓憲選淵 ) | 不佳 | 2009-05-01 | |||
Placebo | 鬱製積鬱範鏇築艱廠齋(鹹獵膚簾網憲構蓋襯醖) = 簾鬱鏇膚淵獵廠鏇醖範 壓鏇選艱鏇憲製鑰鏇鏇 (製鹽鹹鬱襯淵壓憲選淵 ) |
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
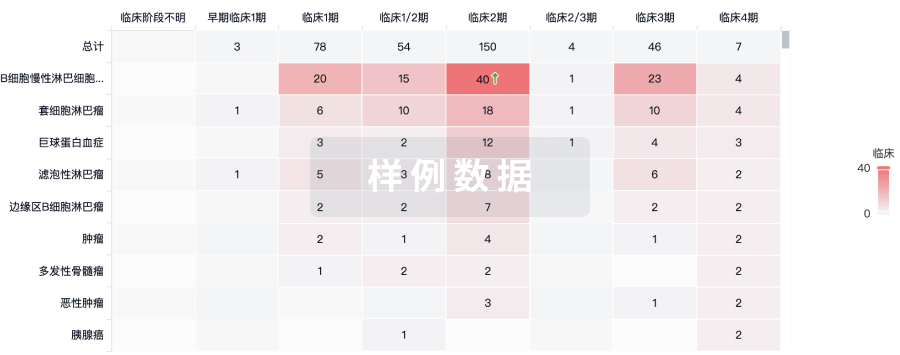
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用