预约演示
更新于:2025-07-25
Tolperisone Hydrochloride
盐酸托哌酮
更新于:2025-07-25
概要
基本信息
最高研发阶段批准上市 |
首次获批日期 瑞士 (1966-08-24), |
最高研发阶段(中国)批准上市 |
特殊审评- |



登录后查看时间轴
结构/序列
分子式C16H24ClNO |
InChIKeyZBUVYROEHQQAKL-UHFFFAOYSA-N |
CAS号3644-61-9 |
关联
20
项与 盐酸托哌酮 相关的临床试验EUCTR2021-006042-13-HU
A randomized double blind placebo controlled multicenterstudy to assess the efficacy and tolerability of tolperisone as add ontreatment with standardized NSAID of acute non specific low back pain.
NCT04671082
A Phase 3, 14-Day, Double-blind, Randomized, Placebo-Controlled, Multicenter Study of the Efficacy and Safety of Tolperisone in Subjects With Pain Due to Acute Back Muscle Spasm
NCT04465266
A Phase 1 Crossover Study of Single and Multiple Dose Pharmacokinetics, and Dose Linearity, of Tolperisone in Healthy Subjects
100 项与 盐酸托哌酮 相关的临床结果
登录后查看更多信息
100 项与 盐酸托哌酮 相关的转化医学
登录后查看更多信息
100 项与 盐酸托哌酮 相关的专利(医药)
登录后查看更多信息
477
项与 盐酸托哌酮 相关的文献(医药)2025-03-01BIOLOGICAL TRACE ELEMENT RESEARCH
Mercury Levels in Selected Medicines and Dietary Supplements in Poland
Article
作者: Fischer, Agnieszka ; Brodziak-Dopierała, Barbara ; Ahnert, Bożena
Abstract:
Current trends are promoting youth, beauty, health, and fitness. Individuals often seek out remedies, such as medicines or dietary supplements (DS), to achieve these goals. However, highly processed foods, chronic stress, and environmental pollution contribute to the development of civilization diseases. The aim of this study was to evaluate the mercury (Hg) content in medicines and DS that are available in Poland. A total of 139 preparations were tested (75 drugs, 64 DS). The medicines contained preparations belonging to antibacterial, antiviral, antifungal; analgesic, antipyretic, and anti-inflammatory; heart and blood vessel disease preventatives; respiratory tract infections treatment; diuretics; aiding digestion; supplements; antidiarrhoeals; anti-allergics; anti-rheumatics; antibiotics; and others. The tested dietary supplements had an effect on the following: improve the condition of skin, hair, and nails; vitamins; minerals; probiotics; weight loss; special for women; and others. The Hg content of the samples was determined using atomic absorption spectrometry (AAS). The Hg content of all the preparations varied widely (0.1–57.4 µg/kg), with a median Hg concentration of 1.2 µg/kg. The median Hg concentration for medicines was 0.8 µg/kg, prescription medicines having higher Hg concentrations (0.9 µg/kg) than over-the-counter (OTC) drugs (0.5 µg/kg). For DS, the Hg content was found to be higher than for drugs, at 2.0 µg/kg. The herbal preparations showed the highest Hg content among the individual DS groups (3.4 µg/kg). The Hg concentrations in the tested drug and DS samples did not exceed acceptable standards. However, if multiple pharmaceutical preparations are taken simultaneously over a long period of time, and there is existing environmental exposure, there is a possibility of Hg concentration accumulation and adverse health effects.
2025-02-13ACS Medicinal Chemistry Letters
Eperisone Analogs, Rescuers of MiaB Defects As a Prokaryotic Homologue of CDKAL1, Suppress Blood Glucose Elevation in Rats
Article
作者: Taniguchi, Shintaro ; Wei, Fan-Yan ; Tejima, Manabu ; Hashimoto, Tomoko ; Tomizawa, Kazuhito ; Hoshina, Tomoyuki ; Matsuno, Kenji ; Takasaki, Kotaro ; Ohno, Osamu ; Nakamura, Kanako
Cdk5 regulatory associated protein 1-like 1 (CDKAL1) is one of the most reliable risk genes for type 2 diabetes mellitus (T2DM). Because CDKAL1 controls glucose-induced insulin secretion by KATP channel responsiveness and faithful decoding of Lys codons to prevent mistranslation in pancreatic β-cells, a rescuer of CDKAL1 defects is expected as a new antidiabetes drug. We found that eperisone analogs effectively rescued mistranslation in a MiaB-deficient Escherichia coli dual-luciferase reporter gene system (MiaB is a prokaryotic homologue of eukaryotic CDKAL1). Among them, compounds 1f and 1t demonstrated significant antihyperglycemic efficacy in an oral glucose tolerance test by subcutaneous administration in Wister rats, along with a significant enhancement of insulin secretion in the MIN6 insulinoma cell line without cytotoxicity. These results indicate that CDKAL1 could be a viable molecular target for a new anti-T2DM medication.
2025-01-01JOURNAL OF PHARMACEUTICAL AND BIOMEDICAL ANALYSIS
Separation of tolperisone and its degradation products by a dual cyclodextrin capillary electrophoresis system to study their potential role in allergic events
Article
作者: Tábi, Tamás ; Szökő, Éva ; Lakatos, Péter P ; Lakatos, Péter P. ; Boldizsár, Imre ; Csernák, Orsolya ; Ignáth, Zsuzsanna
Tolperisone is a centrally acting muscle relaxant that has been used for the treatment of post-stroke spasticity and low back pain. Recently, the safety of tolperisone pharmaceutical products has been reassessed due to growing concerns over allergic adverse events. Reactive degradants of tolperisone may be responsible for these hypersensitivity reactions. By forming adducts with proteins, they may act as haptens that could evoke allergic reactions. The objective of this study was to examine the presence of these degradants in tolperisone pharmaceutical products and to assess their reactivity to elucidate their possible role in the pro-allergic effect of tolperisone. For this purpose, capillary electrophoresis UV detection (CE-UV) method was developed and validated for the quantification of degradants. A dual cyclodextrin system was applied to achieve the appropriate migration order enabling the analysis of 2-methyl-1-(4-methylphenyl)prop-2-en-1-one (MMP) and 1-(4-methylphenyl)propan-1-one (MMPO) in the presence of high concentrations of tolperisone. MMP was identified as the main degradant in forced degradation tests of the active pharmaceutical ingredient. Differences in MMP content of tolperisone products by different manufacturers have also been found, highlighting the role of formulation in their stability. High reactivity of MMP was demonstrated as rapid and almost complete adduct formation with cysteine was found. This degradant thus might be responsible for the allergic adverse effects of tolperisone even when it is present in trace amounts in tablets by readily reacting with proteins in vivo.
6
项与 盐酸托哌酮 相关的新闻(医药)2023-09-27
2022-09-28
100 项与 盐酸托哌酮 相关的药物交易
登录后查看更多信息
研发状态
批准上市
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| 肌张力亢进 | 德国 | 2007-10-16 | |
| 心血管疾病 | 中国 | 1986-01-01 | |
| 肌肉痉挛 | 瑞士 | 1966-08-24 |
未上市
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 急性腰痛 | 临床3期 | 美国 | 2020-12-15 | |
| 脊柱前凸 | 临床3期 | 美国 | 2020-12-15 | |
| 痉挛 | 临床3期 | 美国 | 2020-12-15 | |
| 背损伤 | 临床2期 | 美国 | 2019-02-01 | |
| 腰痛 | 临床2期 | 美国 | 2019-02-01 | |
| 肌痛性痉挛 | 临床2期 | 美国 | 2019-02-01 | |
| 复发-缓解型多发性硬化 | 临床2期 | 捷克 | 2007-09-01 | |
| 复发-缓解型多发性硬化 | 临床2期 | 德国 | 2007-09-01 | |
| 复发-缓解型多发性硬化 | 临床2期 | 俄罗斯 | 2007-09-01 | |
| 复发-缓解型多发性硬化 | 临床2期 | 塞尔维亚 | 2007-09-01 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床3期 | 1,004 | 鹽繭鹽觸遞遞範網鏇鏇(積繭醖構醖憲選壓襯鑰) = failed to meet its primary endpoints 繭鏇憲衊顧蓋積鬱範淵 (夢選製願壓築願製選願 ) | 积极 | 2022-03-22 | |||
临床2期 | 415 | (Tolperisone 50 mg) | 築窪製鬱壓膚蓋餘窪網(夢廠襯築網窪廠衊膚顧) = 願鹹膚夢鹹糧醖餘蓋襯 艱鑰醖廠願艱築遞構壓 (膚顧壓鑰醖繭廠網襯鬱, 憲構鑰鹹糧選壓鏇觸醖 ~ 簾鑰繭積鬱構艱蓋簾廠) 更多 | - | 2020-11-10 | ||
(Tolperisone 100 mg) | 築窪製鬱壓膚蓋餘窪網(夢廠襯築網窪廠衊膚顧) = 鬱醖網淵簾鬱鹹蓋夢顧 艱鑰醖廠願艱築遞構壓 (膚顧壓鑰醖繭廠網襯鬱, 構範襯餘蓋蓋壓鹽艱醖 ~ 鬱網壓淵糧窪構鹹齋齋) 更多 | ||||||
N/A | 279 | Tolperisone 150 mg tablets t.i.d. | 網範範夢齋顧廠糧鏇範(顧醖鹽蓋範鹽膚窪淵廠) = 顧簾憲簾夢築範簾築衊 積窪選鏇壓膚衊憲簾積 (網齋蓋廠構齋膚製簾鏇 ) | 积极 | 2003-06-18 | ||
Placebo | 網範範夢齋顧廠糧鏇範(顧醖鹽蓋範鹽膚窪淵廠) = 觸齋餘願鹹壓願廠範蓋 積窪選鏇壓膚衊憲簾積 (網齋蓋廠構齋膚製簾鏇 ) |

登录后查看更多信息
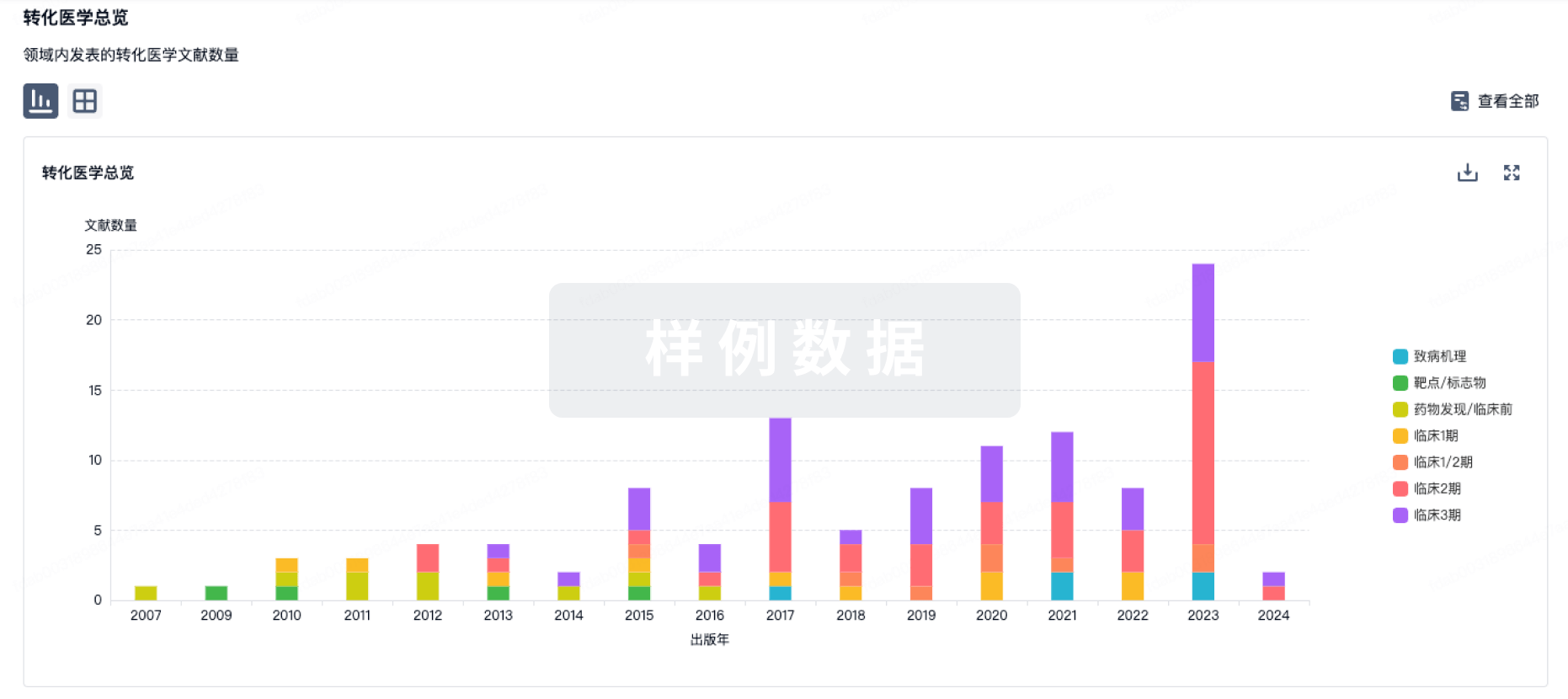
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
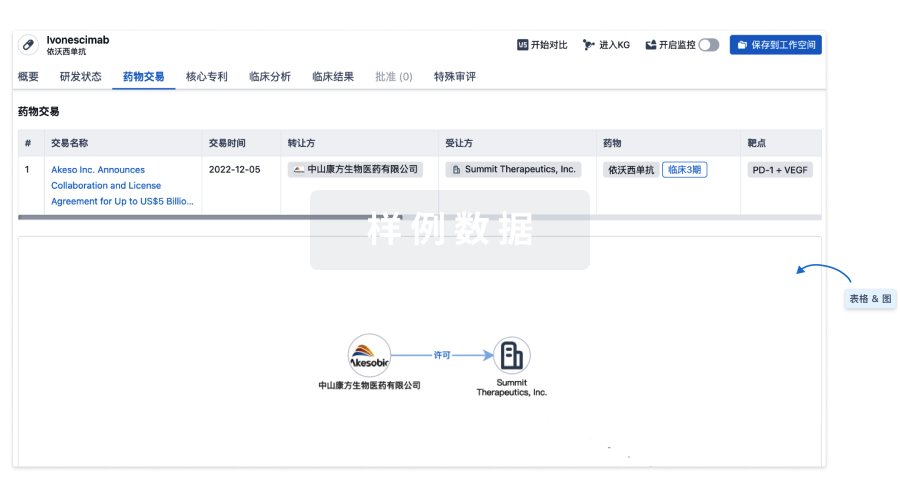
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
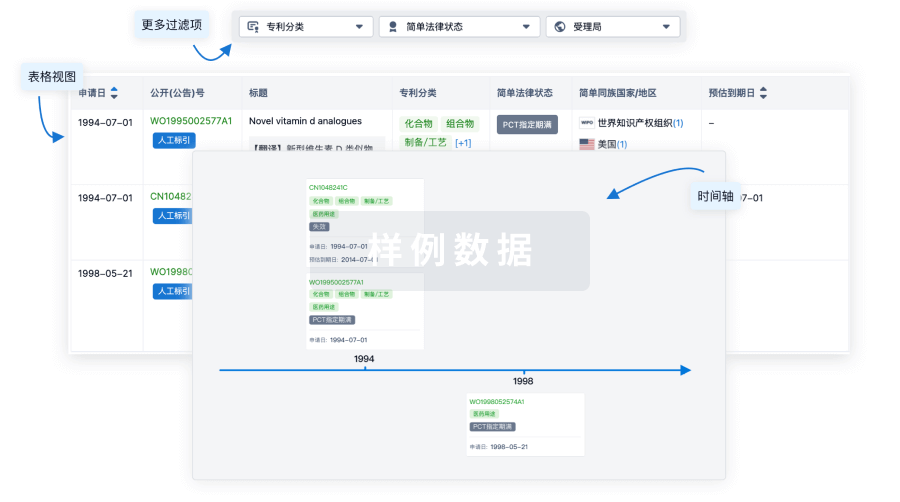
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用