预约演示
更新于:2025-08-23
Levobetaxolol Hydrochloride
盐酸左倍他洛尔
更新于:2025-08-23
概要
基本信息
药物类型 小分子化药 |
别名 (S)-betaxolol、Levobetaxolol、Levobetaxolol hydrochloride (USAN) + [5] |
作用方式 拮抗剂 |
作用机制 β1-adrenergic receptor拮抗剂(β1-肾上腺素能受体拮抗剂) |
治疗领域 |
在研适应症- |
原研机构 |
在研机构- |
权益机构- |
最高研发阶段撤市 |
最高研发阶段(中国)无进展 |
特殊审评- |

登录后查看时间轴
结构/序列
分子式C18H30ClNO3 |
InChIKeyCHDPSNLJFOQTRK-LMOVPXPDSA-N |
CAS号116209-55-3 |
关联
4
项与 盐酸左倍他洛尔 相关的临床试验CTR20171325
盐酸左倍他洛尔滴眼液治疗原发性开角型青光眼、高眼压症随机、开放性、阳性药平行对照、多中心临床试验
CTR20170010
盐酸左倍他洛尔滴眼液治疗原发性开角型青光眼、高眼压症随机、盲法、阳性药平行对照、多中心临床试验
CTR20150505
盐酸左倍他洛尔滴眼液治疗原发性开角型青光眼、高眼压症随机、单盲、阳性药平行对照、多中心临床试验
100 项与 盐酸左倍他洛尔 相关的临床结果
登录后查看更多信息
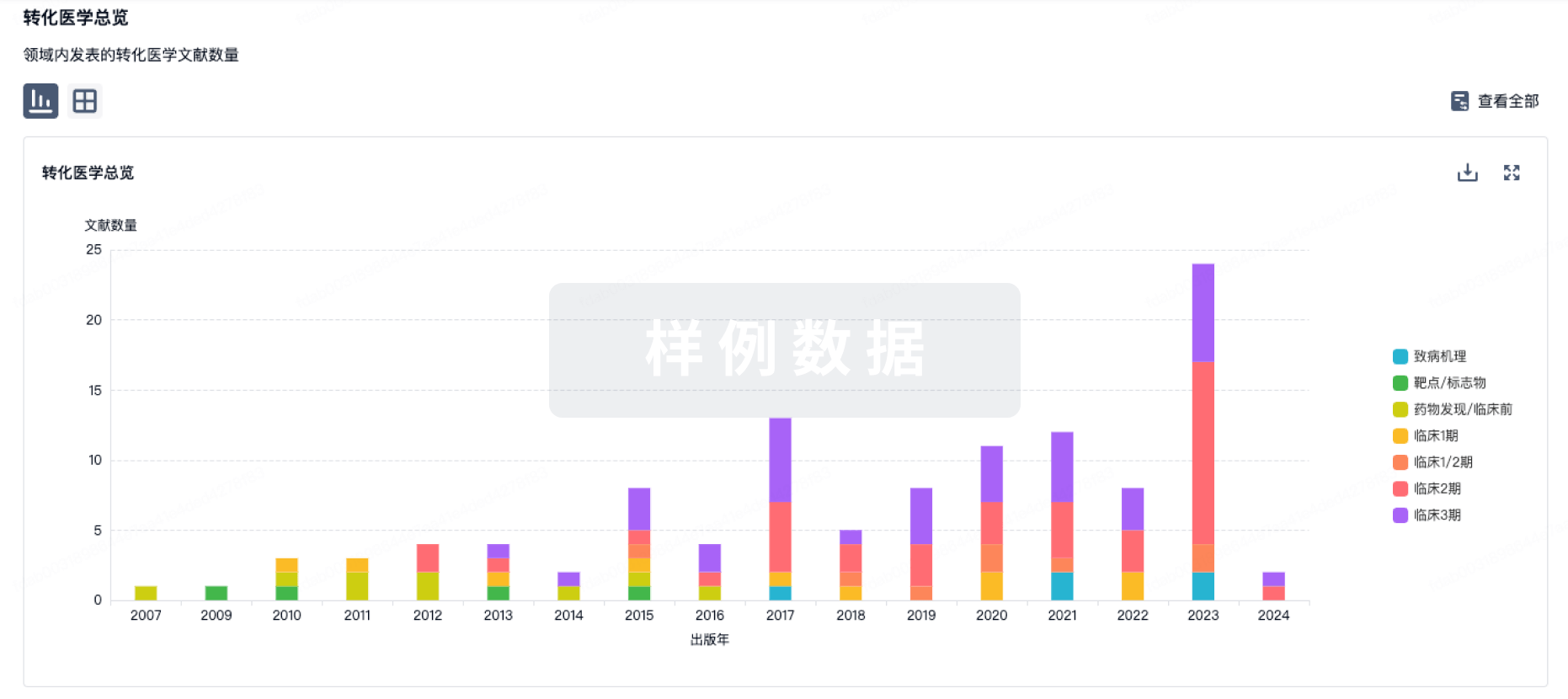
100 项与 盐酸左倍他洛尔 相关的转化医学
登录后查看更多信息
100 项与 盐酸左倍他洛尔 相关的专利(医药)
登录后查看更多信息
78
项与 盐酸左倍他洛尔 相关的文献(医药)2024-08-01ARCHIVES OF BIOCHEMISTRY AND BIOPHYSICS
Investigation of F508del CFTR unfolding and a search for stabilizing small molecules
Article
作者: Meng, Xin ; Ford, Robert C
Mutation of phenylalanine at position 508 in the cystic fibrosis transmembrane conductance regulator (F508del CFTR) yields a protein unstable at physiological temperatures that is rapidly degraded in the cell. This mutation is present in about 90% of cystic fibrosis patients, hence there is great interest in compounds reversing its instability. We have previously reported the expression of the mutated protein at low temperature and its purification in detergent. Here we describe the use of the protein to screen compounds present in a library of Federal Drug Administration (FDA) - approved drugs and also in a small natural product library. The kinetics of unfolding of F508del CFTR at 37 °C were probed by the increase in solvent-exposed cysteine residues accessible to a fluorescent reporter molecule. This occurred in a bi-exponential manner with a major (≈60%) component of half-life around 5 min and a minor component of around 60 min. The faster kinetics match those observed for loss of channel activity of F508del CFTR in cells at 37 °C. Most compounds tested had no effect on the fluorescence increase, but some were identified that significantly slowed the kinetics. The general properties of these compounds, and any likely mechanisms for inducing stability in purified CFTR are discussed. These experimental data may be useful for artificial intelligence - aided design of CFTR-specific drugs and in the identification of stabilizing additives for membrane proteins (in general).
2020-08-01Graefe's Archive for Clinical and Experimental Ophthalmology
Medical management of pediatric glaucoma: lessons learned from randomized clinical trials
Review
作者: Lucentini, Stefano ; Nucci, Paolo ; Lizzio, Rosario Alfio Umberto ; Serafino, Massimiliano ; Villani, Edoardo ; Sacchi, Matteo ; Monsellato, Gianluca ; Luccarelli, Saverio ; Cremonesi, Elena
PURPOSE:
To critically discuss the randomized clinical trials (RCTs) on glaucoma medical therapy for the management of pediatric glaucoma.
METHODS:
RCTs on glaucoma drugs carried out on pediatric subjects with ocular hypertension and glaucoma were identified through systematic searches. The methods of the RCTs and the safety and the efficacy of the glaucoma drugs were reviewed and discussed.
RESULTS:
We included five RCTs. One study compared dorzolamide with 0.5% timolol gel; one brinzolamide with 0.5% levobetaxolol; one 0.25% betaxolol, 0.25% timolol gel, and 0.5% timolol gel; one latanoprost with 0.5% timolol; and one travoprost with 0.5% timolol. The primary outcome was safety for two studies and efficacy for three studies. None of the RCTs was powered to detect statistically significant differences in intraocular pressure (IOP) between treatments. In total, 658 subjects received at least one dose of study medication. Beta-blockers were administered to 359 patients, carbonic anhydrase inhibitor (CAI) to 154, and prostaglandins to 145 patients. IOP-lowering efficacy ranged from 20 to 23% for CAI, from 9 to 36% for beta-blockers, and from 26 to 27% for prostaglandins. The percentage of responders was 50% for CAI, ranged from 38 to 74% for beta-blockers and from 60 to 83% for prostaglandins. Two patients receiving timolol experienced a systemic, drug-related serious adverse event (one patient bradycardia and one pneumonia). Systemic, nonserious drug-related events occurred in 15 patients randomized to beta-blockers and in 8 patients randomized to CAI. No adverse events occurred in children treated with prostaglandins.
CONCLUSION:
RCTs that are available on medical therapy for glaucoma are few and underpowered. The proportion of responders is lower in children; however, in subjects who are responders, the efficacy of glaucoma drugs seemed to be comparable to that in adults. As systemic adverse events have been reported, including serious events with timolol, a particular attempt to minimize the absorption of the drug (using the lowest dose and the gel formulation of beta-blockers or considering the lacrimal punctum occlusion) and a follow-up that is more frequent and more focused on safety should be considered in pediatric subjects who are on topical glaucoma medications.
2019-04-01Analytical and Bioanalytical Chemistry
Enantioseparation of chiral β-blockers using polynorepinephrine-coated nanoparticles and chiral capillary electrophoresis
Article
作者: Xiao, Xue ; Jia, Li ; Li, Zhenqun ; Wu, Jia
A method of combining magnetic solid-phase separation (MSPE) and chiral capillary electrophoresis (CE) is developed for enantioseparation of trace amounts of β-blockers. Polynorepinephrine-functionalized magnetic nanoparticles (polyNE-MNPs) are synthesized and applied to simultaneously extract three β-blockers (carteolol, metoprolol, and betaxolol). The prepared polyNE-MNPs are spherical with a diameter of 198 ± 17 nm and the thickness of the polyNE coating is about 14 nm. PolyNE possesses abundant catechol hydroxyl and secondary amine groups, endowing the MNPs with excellent hydrophilicity. Under the optimum conditions, the extraction efficiencies of polyNE-MNPs for β-blockers are in the range of 89.6 to 100%, with relative standard deviations (RSDs) below 3.5%. The extraction process can be finished in 4 min. Field-enhanced sample injection (FESI) in chiral CE is constructed to further enhance the sensitivities of β-blocker enantiomers. The limits of detection for β-blocker enantiomers by the FESI-CE with polyNE-MNPs are in the range of 0.401 to 1.59 ng mL-1. The practicability of this method in real samples is evaluated by analysis of human urine samples. The recoveries for each enantiomer of β-blockers in the real samples range from 89.5 to 92.8%, with RSDs ranging from 0.37 to 5.9%. The whole detection process can be finished in less than 0.5 h. The method demonstrates its great potential in the pharmacokinetic and pharmacodynamic studies of chiral drugs in humans. Graphical abstract ᅟ.
100 项与 盐酸左倍他洛尔 相关的药物交易
登录后查看更多信息
研发状态
批准上市
10 条最早获批的记录, 后查看更多信息
登录
| 适应症 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|
| 开角型青光眼 | 美国 | 2000-02-23 | |
| 高眼压症 | 美国 | 2000-02-23 |
未上市
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 青光眼 | 临床3期 | - | 2003-01-01 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
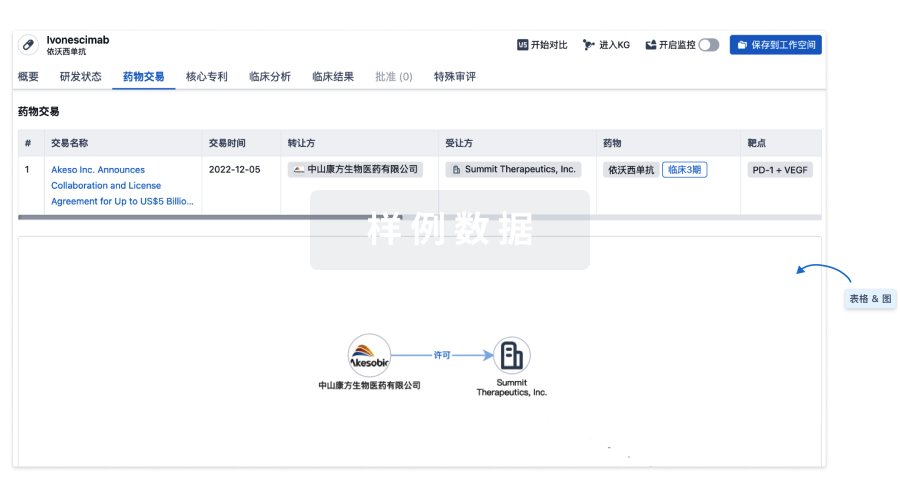
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
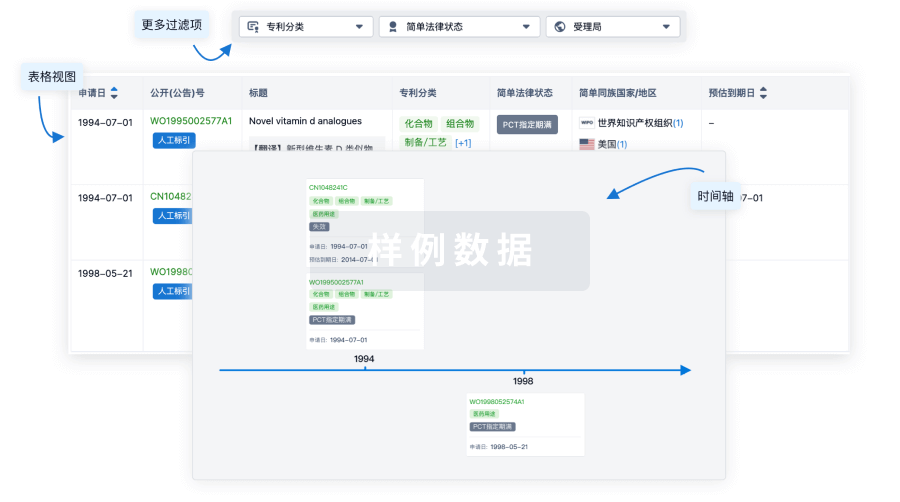
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用