预约演示
更新于:2025-05-07

IQVIA, Inc.
更新于:2025-05-07
概览
关联
DRKS00035925
VONKO-027: Development and application of a therapy line algorithm, evaluation of data completeness and estimation of the number of patients in a SCLC population within the existing lung cancer cohort from the VONKO-001 project - VONKOdb extensive stage SCLC 2025
DRKS00035340
Clinical characteristics, treatment patterns and survival of individuals with adenocarcinoma of the stomach (ICD-10 C16) or the gastro-oesophageal junction (ICD-10 C15.5) in Germany - a study based on cancer registry data (VONKO-022) - VONKOdb GC 2024
NCT06716801
Observational Cohort Study on Adult Patients with Not-adequately Controlled FOcal-onset Seizures Treated with Cenobamate As Early AdjUnctive Therapy in a Real-world Setting - FOCUS

100 项与 IQVIA, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-05-01European Urology
Effects of Enzalutamide on the Sexual Activity of Patients with Biochemically Recurrent Prostate Cancer: A Post Hoc Analysis of Patient-reported Outcomes in the EMBARK Study
Article
作者: Freedland, Stephen J ; Mulhall, John P ; Reisman, Arlene L ; Shore, Neal ; Ivanova, Jasmina I ; Saad, Fred ; Nasr, Anchen F ; Ganguli, Arijit ; Turnbull, James ; Kral, Pavol ; Gleave, Martin ; Giorgi, Ugo De ; Rannikko, Antti
2025-03-01Clinical Microbiology and Infection
Performance of molecular tests for diagnosis of bloodstream infections in the clinical setting: a systematic literature review and meta-analysis
Review
作者: Wang, Yu ; Lindsley, Kristina ; Gu, Yifan ; Uyei, Jennifer ; Timbrook, Tristan T ; Jiudice, Sarah ; Wang, Yi ; Balada-Llasat, Joan-Miquel ; Bleak, Tammy C
2025-03-01PharmacoEconomics - Open
Clinical Complications and Healthcare Resource Utilization Associated with Conventional Management of Sickle Cell Disease with Recurrent Vaso-occlusive Crises and Transfusion-Dependent β-Thalassemia in Germany
Article
作者: Meisel, Roland ; Tuzin, Petra ; Alba, Aranzazu ; Dombrowski, Silvia ; Baldwin, Jessica ; Li, Nanxin ; Georgiadou-Schmidt, Elena ; Kunzweiler, Colin ; Zingel, Sebastian Dietmar ; Udeze, Chuka ; Vetter, Céline

2025-04-30
生物类似药引进/卖出临床1期抗体药物偶联物临床3期
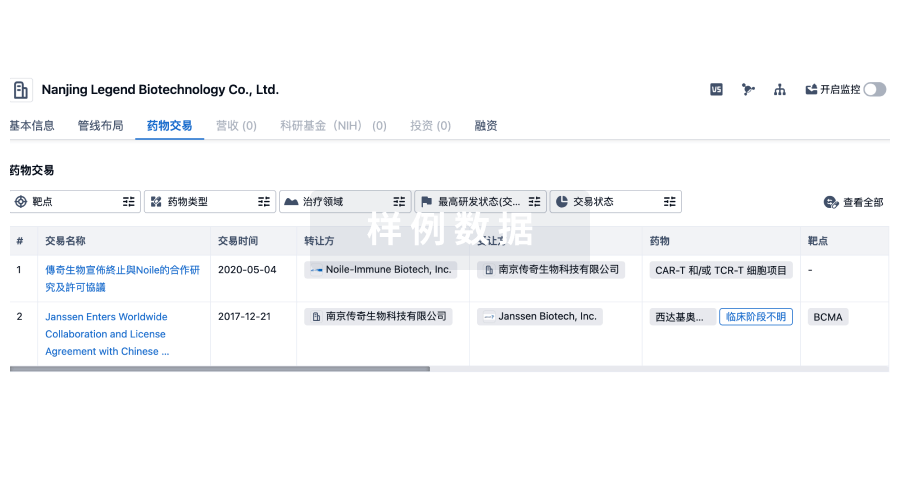
100 项与 IQVIA, Inc. 相关的药物交易
登录后查看更多信息
100 项与 IQVIA, Inc. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年09月02日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
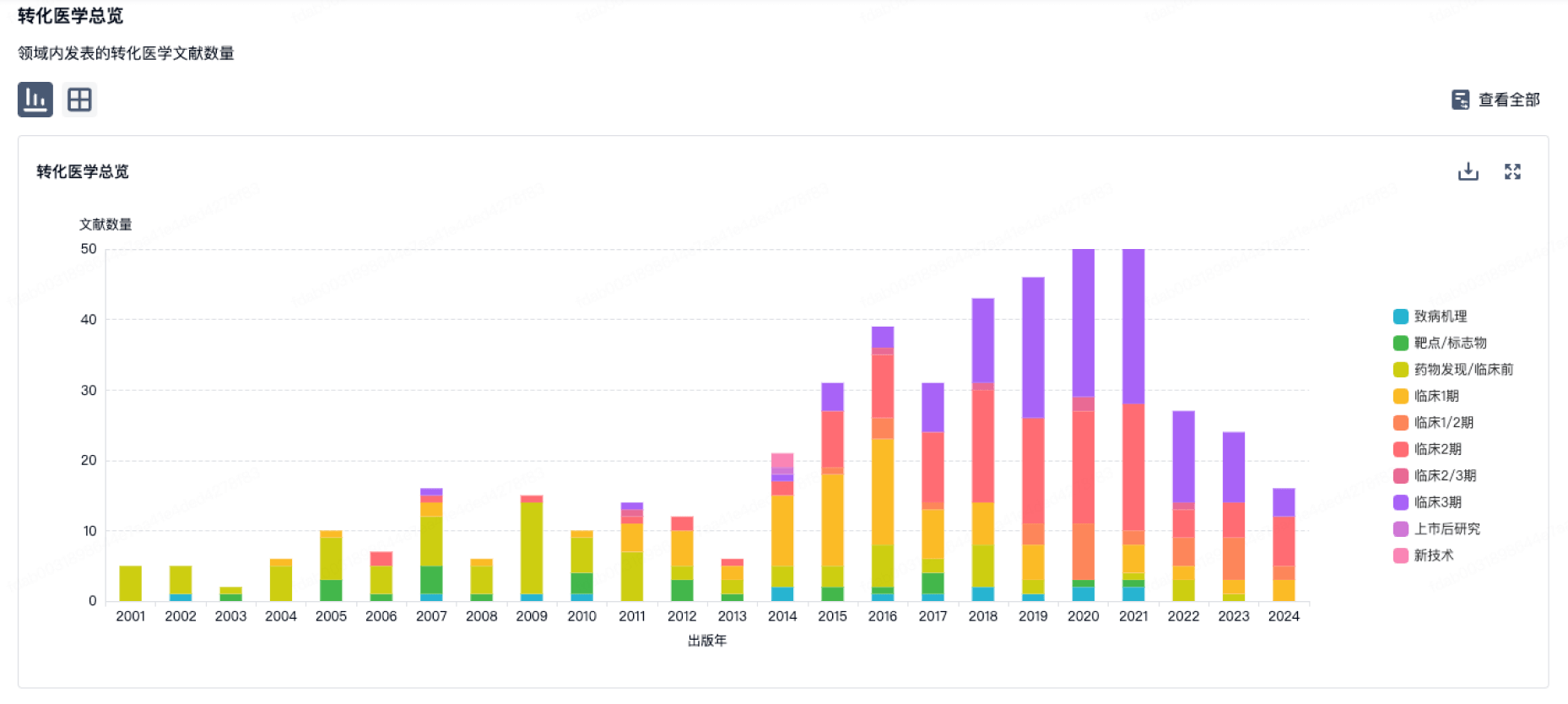
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
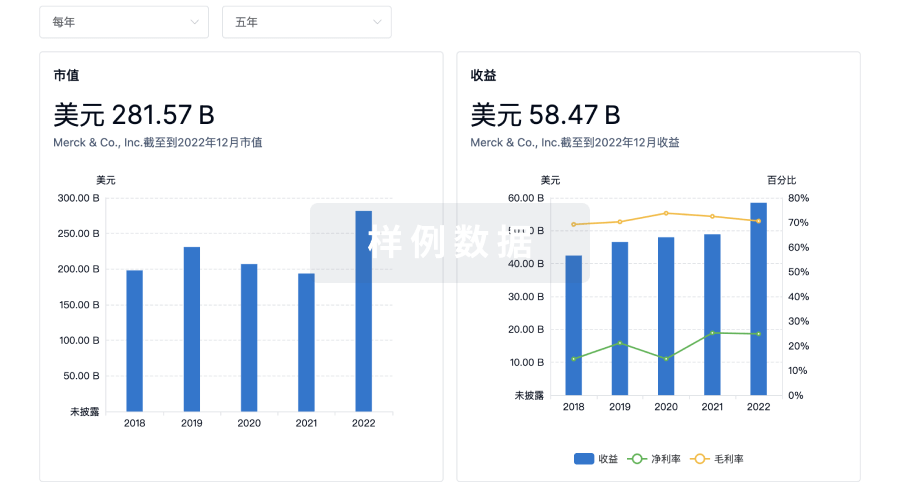
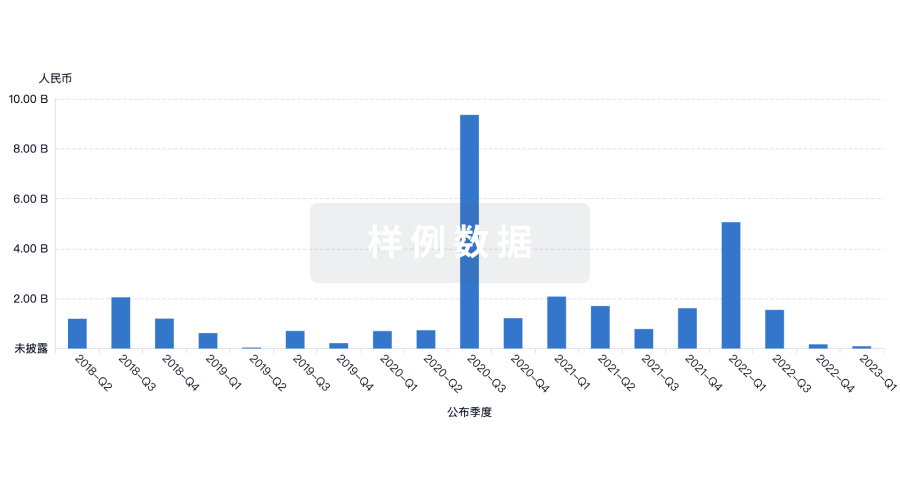
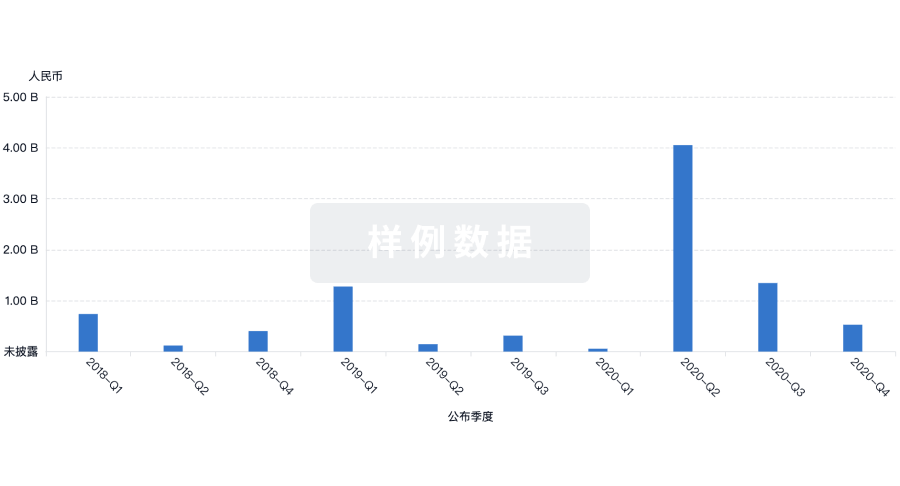
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用