预约演示
更新于:2025-03-09

AstraZeneca Pharma India Ltd.
更新于:2025-03-09
概览
关联
42
项与 AstraZeneca Pharma India Ltd. 相关的临床试验CTRI/2024/11/076716
A Double-Blind, Randomized, Placebo-Controlled, Multicentre Study Evaluating the Efficacy and Safety of Baxdrostat in Asian Participants with Uncontrolled Hypertension on Two or More Medications including Participants with Resistant Hypertension (BAXASIA)
开始日期2024-11-23 |
申办/合作机构 AstraZeneca AB [+1] |
CTRI/2024/09/073943
A Phase III, Randomised, Double -Blind, Active-controlled Study to Assess the Efficacy, Safety and Tolerability of Baxdrostat in Combination with Dapagliflozin Compared with Dapagliflozin Alone on Chronic Kidney Disease (CKD) Progression in Participants with CKD and High Blood Pressure (BaxDuo ARCTIC)
开始日期2024-10-01 |
申办/合作机构 AstraZeneca AB [+1] |
CTRI/2024/07/071759
A Study to Identify and Characterise Patients with Chronic Kidney Disease and Proteinuria - NIL
开始日期2024-08-10 |
申办/合作机构 AstraZeneca AB [+1] |
100 项与 AstraZeneca Pharma India Ltd. 相关的临床结果
登录后查看更多信息
0 项与 AstraZeneca Pharma India Ltd. 相关的专利(医药)
登录后查看更多信息
34
项与 AstraZeneca Pharma India Ltd. 相关的文献(医药)2024-11-05·Cureus Journal of Medical Science
Harnessing Digital Initiatives for Improved Health Outcomes in Diabetes Management: An Observational Patient Program
Article
作者: Baruah, Manash ; Sada, Prashant ; Deshmukh, Vaishali ; Seshadri, Krishna ; Ag, Unnikrishnan ; Aggarwal, Khushboo ; Sethi, Bipin ; Hs, Bharath ; Ghosal, Samit ; Chittawar, Sachin ; Phatak, Sanjeev
INTRODUCTION:
Patients with diabetes have easy access to a wide range of digital applications that may help with self-management and lower barriers; however, robust evidence of their effectiveness remains somewhat elusive. Zyla is a medical artificial intelligence (AI)-based personalized care management app that assists the treating physician in improving the standard of patient care by offering the patients comprehensive and individualized care. This preliminary evaluation of data collected through the Zyla app aims to understand the impact of diabetes disease outcomes among patients subscribed to this app.
METHODS:
This was a retrospective, observational program conducted through the Zyla app in the calendar year 2020. The Zyla app's objective is to assist the treating physician in improving the standard of patient care by giving them the choice of assembling a personalized team (consisting of clinical nutritionists, physiotherapists, and counselors over a virtual platform) that can offer patients comprehensive and individualized care. Data on parameters like glycated hemoglobin (HbA1c), fasting blood sugar (FBS), post-prandial glucose (PPG), serum creatinine (SC), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C) and low-density lipoprotein cholesterol (LDL-C) were collected through the Zyla app. Clinical outcomes assessed were the change from baseline to last reported levels of the mentioned parameters and are reported using descriptive analysis.
RESULTS:
The glycemic control parameters, HbA1c (change from baseline (CFB): -1.08), FBS (CFB: -15.93), and PPG levels (-18.42), were significantly lower (P<0.0001) at the last assessment compared with baseline. For the lipid profile, levels of TGs (P<0.0001) and TC (P = 0.0037) were significantly lower compared with baseline, while HDL-C levels were comparatively higher (CFB: 0.68) and LDL-C levels were lower (CFB:11.60), however non-significant. Serum creatinine was also lower compared to baseline (CFB: -0.25); however, the difference was not statistically significant.
CONCLUSIONS:
A significant improvement in all glycemic parameters was seen with the use of the Zyla app along with numerical improvements in kidney function parameters and cholesterol status among patients. These preliminary findings warrant further rigorous studies to validate the impact of medical apps in the management of diabetics in India.
2024-07-01·Indian Journal of Public Health
Current Practices in Genetic Testing for Prostate Cancer: The Indian Scenario
Article
作者: Baxi, Hemang ; Kulkarni, Utkarsha ; Joshi, Amit ; Bakshi, Ganesh ; Shingla, Shivam ; Talwar, Vineet ; Desai, Chirag ; Mohapatra, Prabrajya Narayan ; Addla, Sanjai ; Rajappa, Senthil
Abstract:
Background::
Despite genetic testing being recommended by international guidelines for the selection of targeted therapy for prostate cancer (PCa), limited data are available on genetic testing for PCa in India.
Objectives::
The objective is to understand the current genetic testing practice pattern for PCa in India.
Materials and Methods::
A panel of 9 experts developed and validated a premeeting online questionnaire comprising 12 objective questions. The questionnaire was circulated from February 2022 to May 2022 among medical oncologists and uro-oncologists across pan-India, followed by response collection over 3 months. Descriptive statistics were used to summarize results and concluding statements were formulated on current genetic testing practice patterns for PCa.
Results::
A total of 103 responses were received. Genetic testing was advised by 35.9% of the participants in <5% of patients with PCa. Patients with a family history of PCa (88.3%) were most commonly referred for genetic testing. Nearly half (50.2%) of the participants routinely tested for homologous recombination repair (HRR) genes; 52% used blood and tissue as the most preferred specimen for performing genetic testing and 44.7% followed the testing sequence of tumor tissue followed by blood. Major barriers to genetic testing were affordability and scarcity of genetic counselors, while a major change could be brought by making it cost-effective and improving access to medication.
Conclusions::
We observed a lower prescription frequency of genetic testing for the HRR gene across pan-India. Improving the quality and access to genetic testing and the availability of cost-effective-targeted therapies will aid in delivering personalized care to patients with metastatic PCa.
2023-11-01·Indian heart journal
Prevalence of cardiac abnormalities and heart failure in unselected out-patients with type 2 diabetes mellitus and associated clinical factors: Real-world evidence from an Indian registry
Article
作者: Rajput, Rajesh ; Dalal, Jamshed ; Mohan, J C ; Kumar, Amit ; Hs, Bharath ; Vasnawala, Hardik ; Mullasari, Ajit ; Sawhney, J P S ; Sarda, Shital
OBJECTIVE:
Type 2 diabetes mellitus (T2DM) is known to be associated with development of left ventricular (LV) dysfunction and heart failure (HF). The study aimed to determine the prevalence of LV dysfunction and HF in unselected out-patients with T2DM with no previous cardiac history and to correlate LV dysfunction and HF with demographic and comorbid characteristics.
METHODS:
This cross-sectional study conducted at 27 centers in India captured demographic and clinical data through electronic case record forms. B-type natriuretic peptide of >105 pg/mL was used to diagnose HF and two-dimensional echocardiography was used to assess LV dysfunction.
RESULTS:
Of the 615 patients, 54.3 % (n = 334) were males; mean age was 57.4 ± 10.48 years. More than one-third of the patients had T2DM duration of >10 years (n = 238; 38.7 %), with hypertension as the most prevalent comorbidity (n = 372, 78.6 %). Approximately 61.3 % of the patients had LV hypertrophy. The mean LV mass was 135.0 ± 56.16 g (95 % CI 130.28, 139.70). The prevalence of any type of LV dysfunction, including systolic or diastolic dysfunction and HF was 55 % (95 % CI 51.0, 59.0) and 10 % (95 % CI 7.0, 12.0), respectively. A negligible but statistically significant correlation was observed between LV dysfunction and T2DM duration (p = 0.011), alongside HF and age (p < 0.0001).
CONCLUSION:
Real-world data from this registry from India demonstrates a substantial burden of LV dysfunction and HF in individuals with T2DM in India. It is imperative to formulate strategies for early identification of LV dysfunction in individuals with T2DM for prevention and consequent management of HF.
2
项与 AstraZeneca Pharma India Ltd. 相关的新闻(医药)2025-03-04
AstraZeneca Pharma India Ltd has received crucial approval from the Central Drugs Standard Control Organisation (CDSCO) to import and distribute its cancer treatment medication, Durvalumab. This announcement was made on March 3, 2025, paving the way for the marketing of this critical therapy in the Indian market.
The CDSCO has granted permission for the infusion solutions of Durvalumab, available in 120 mg/2.4 ml and 500 mg/10 ml formulations, known commercially as Imfinzi. This approval allows AstraZeneca to promote Durvalumab in combination with Tremelimumab for treating patients with unresectable hepatocellular carcinoma (uHCC).
This regulatory clearance is a significant milestone for AstraZeneca as it expands its oncology portfolio in India, addressing the needs of patients suffering from this aggressive form of liver cancer. The company is now set to proceed with marketing these solutions, contingent upon obtaining all necessary statutory approvals.
As the demand for effective cancer treatments continues to rise, AstraZeneca’s expansion of its offerings in India underscores its commitment to improving healthcare outcomes for patients battling cancer.
上市批准
2023-11-17
AstraZeneca has operated in India since 1979.
Amid a corporate review of AstraZeneca’s global manufacturing and supply network, the company’s Indian subsidiary is planning to close up shop at the “beating heart” of its India operations in Bangalore.
AstraZeneca Pharma India will exit its production plant in Bangalore, India, “in due course,” the company said in a filing on the Bombay Stock Exchange Thursday.
AZ plans to auction off the site “in a fully operational manner” to a buyer who can also serve as a contract manufacturer for the AstraZeneca drugs made and packaged in Bangalore, AZ’s Indian subsidiary said.
In the filing, AZ said it is "fully cognizant of the impact this change can bring," adding that the company's "first responsibility will be towards its employees and meeting the needs of its patients by ensuring an uninterrupted supply of medicines."
AstraZeneca has operated in India since 1979, the company says on its website. Aside from its tablet production facility in Bangalore, AZ also operates a global technology center in Chennai, which boasts a workforce of more than 2,300 IT professionals and experts.
The Bangalore facility, for its part, housed more than 900 employees as of mid-August, Narayan Seshadri, AstraZeneca Pharma India’s board chair, said at the company’s annual general meeting this past summer.
The Bangalore site supports 51 global AZ brands and is the headquarters for the Indian company’s commercial operations, AstraZeneca Pharma India added. The site also houses manufacturing and clinical operations. AZ describes the Bangalore plant as the “beating heart” of its India operations.
AZ’s plan to exit its Bangalore site comes after the company announced layoffs of 103 sales staffers in its Indian primary care division back in March. At the time, the employees pushed back against what they described as unlawful terminations, according to local publication The Hindu.
In a statement to Fierce Pharma, AstraZeneca attributed the decision to its evolving “strategic priorities.”
Last year, meanwhile, AstraZeneca locked in a sale of its West Chester, Ohio, site to biomanufacturing outfit National Resilience. Much like the plan in Bangalore, Resilience and AZ forged a long-term agreement under which Resilience is expected to continue producing “select AstraZeneca medicines."
More than 500 employees who worked at AZ’s Ohio facility were set to maintain their jobs after Resilience took control, Andrew Wirths, senior vice president of AstraZeneca’s Americas supply region, said in a statement last fall.
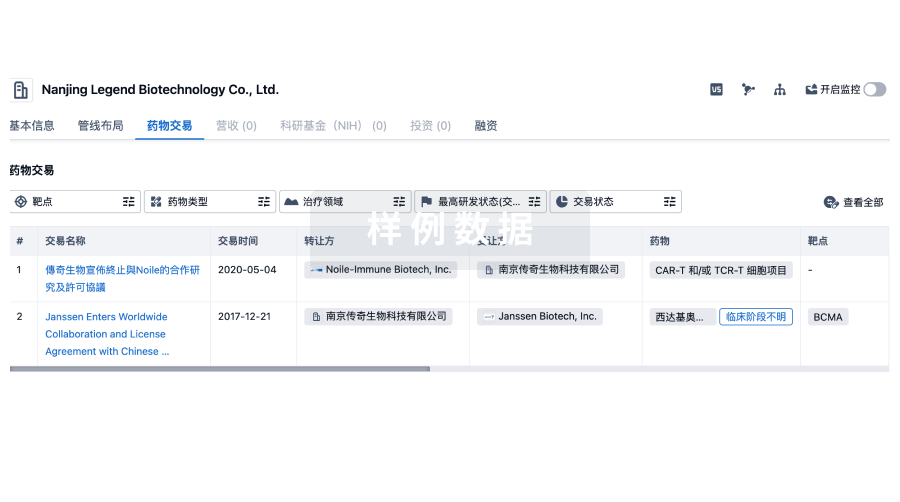
100 项与 AstraZeneca Pharma India Ltd. 相关的药物交易
登录后查看更多信息
100 项与 AstraZeneca Pharma India Ltd. 相关的转化医学
登录后查看更多信息
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年04月20日管线快照
管线布局中药物为当前组织机构及其子机构作为药物机构进行统计,早期临床1期并入临床1期,临床1/2期并入临床2期,临床2/3期并入临床3期
其他
4
登录后查看更多信息
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
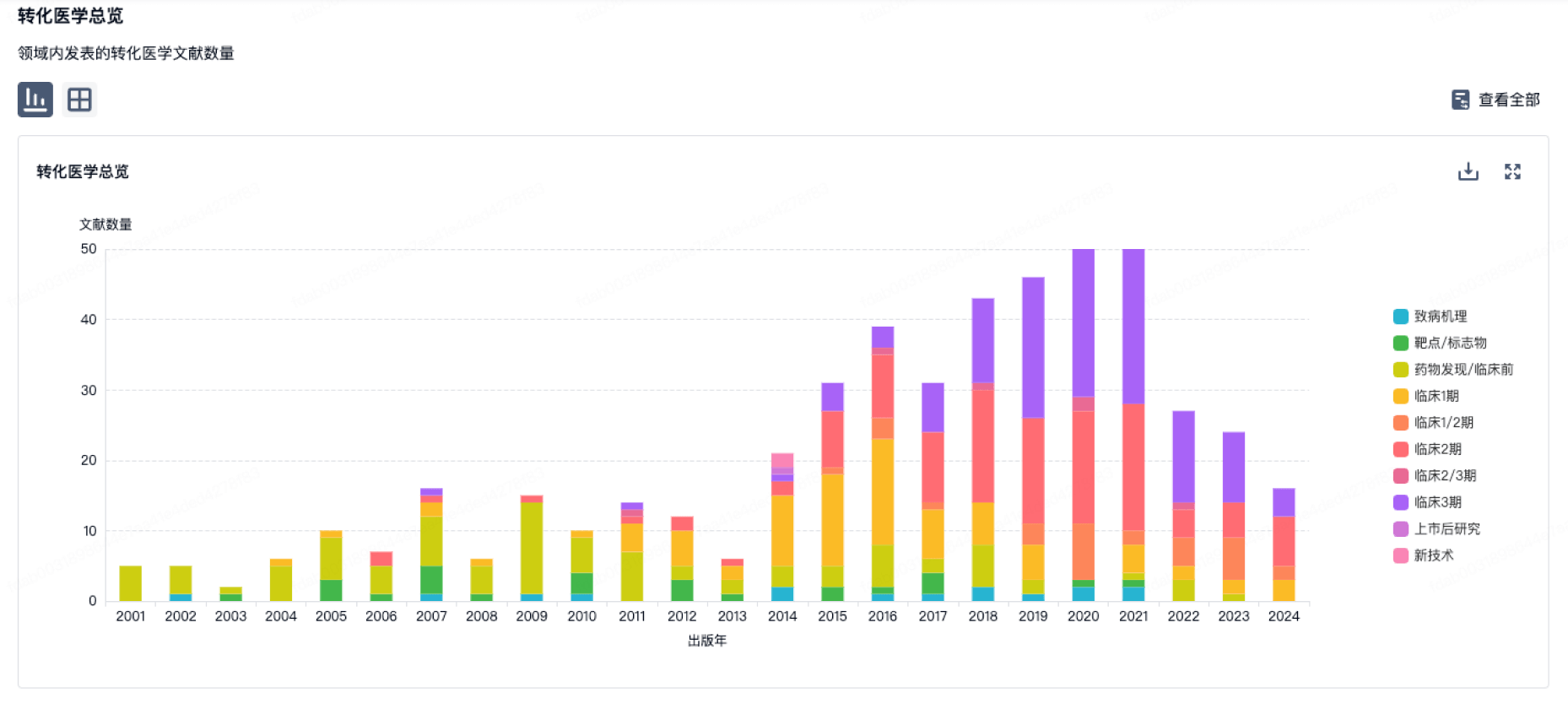
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
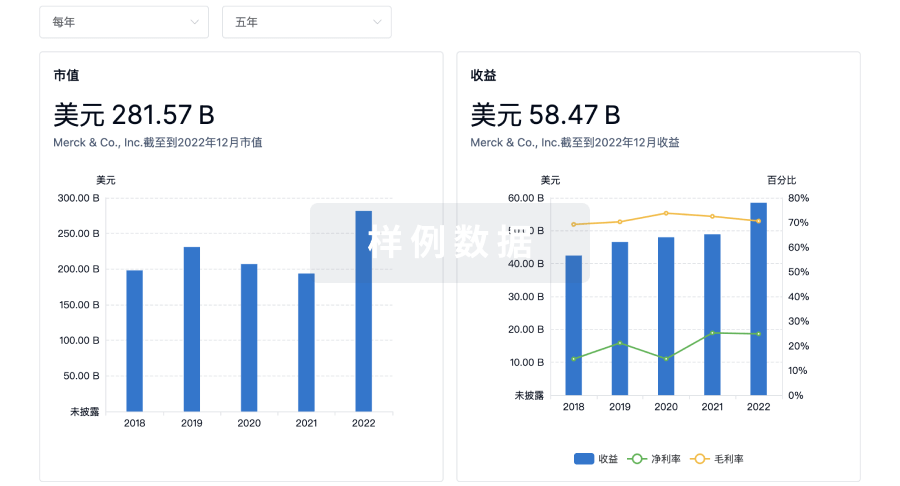
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
来和芽仔聊天吧
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用