预约演示
更新于:2025-05-07

Blue Cross & Blue Shield of North Carolina
更新于:2025-05-07
概览
关联
NCT05048836
Healthy Food First
100 项与 Blue Cross & Blue Shield of North Carolina 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-03-01Journal of managed care & specialty pharmacy
Evaluating the uptake of a Global Initiative for Asthma guideline update in a commercially insured, value-based care population.
Article
作者: Smith, Spenser ; McInturff, Lindsey M
2024-02-01The Gerontologist
Implementation Lessons Learned: Distress Behaviors in Dementia Intervention in Veterans Health Administration
Article
作者: Wray, Laura O ; Karel, Michele J ; Curyto, Kim ; Jedele, Jenefer M ; Sullivan, Jennifer L ; Minor, Lisa ; McConnell, Eleanor S
2023-12-26Journal of the Pediatric Infectious Diseases Society
Trends in Pediatric Emergency and Inpatient Healthcare Use for Mental and Behavioral Health Among North Carolinians During the Early COVID-19 Pandemic
Article
作者: Brookhart, M Alan ; Zimmerman, Kanecia O ; CoyneSmith, Taran ; Charles, Catherine O ; Darden, Toni ; Benjamin, Daniel K ; Sielaty, Rachel ; Boutzoukas, Angelique E ; Overman, Robert A ; Caison, Bria
100 项与 Blue Cross & Blue Shield of North Carolina 相关的药物交易
登录后查看更多信息
100 项与 Blue Cross & Blue Shield of North Carolina 相关的转化医学
登录后查看更多信息
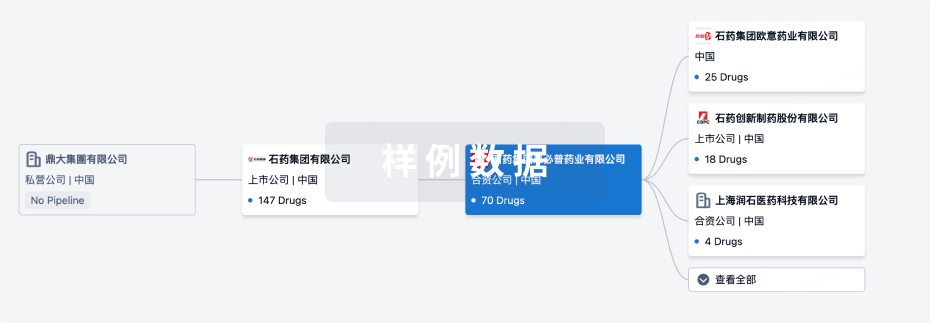
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年07月06日管线快照
无数据报导
登录后保持更新
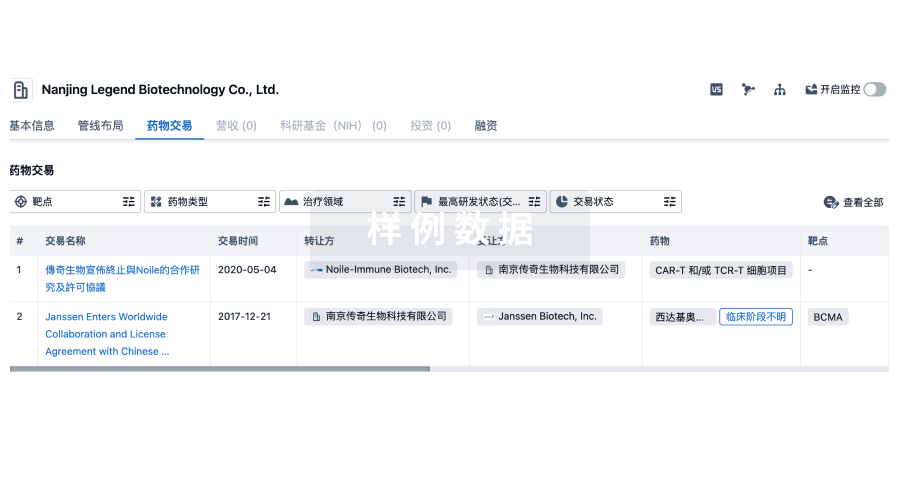
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
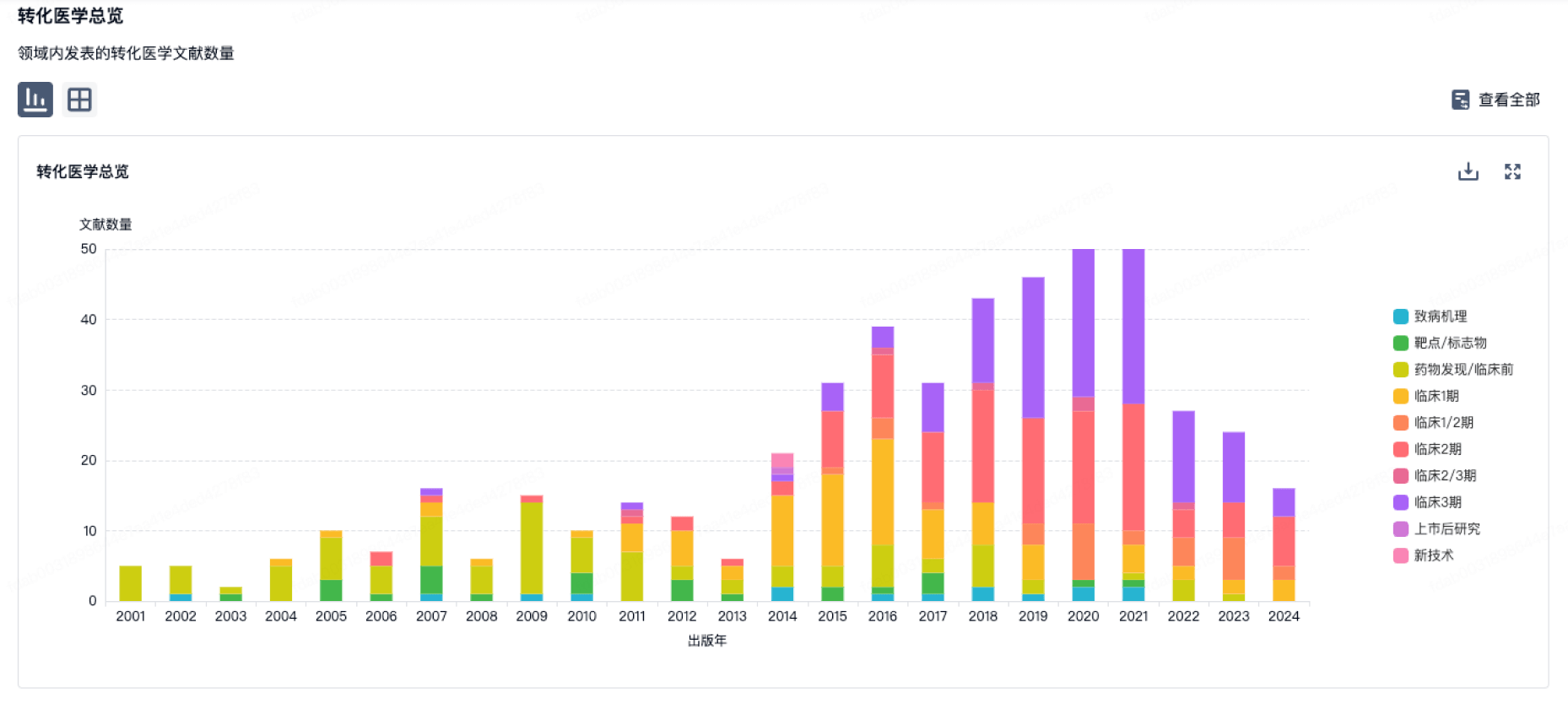
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
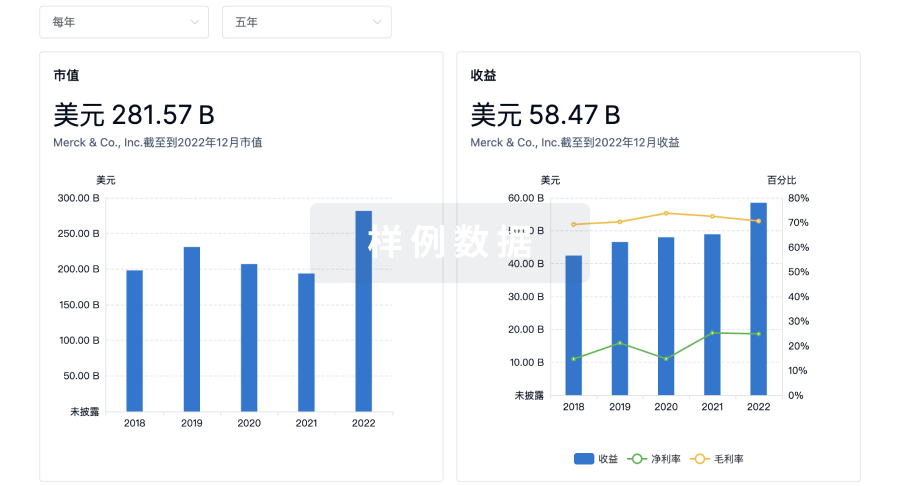
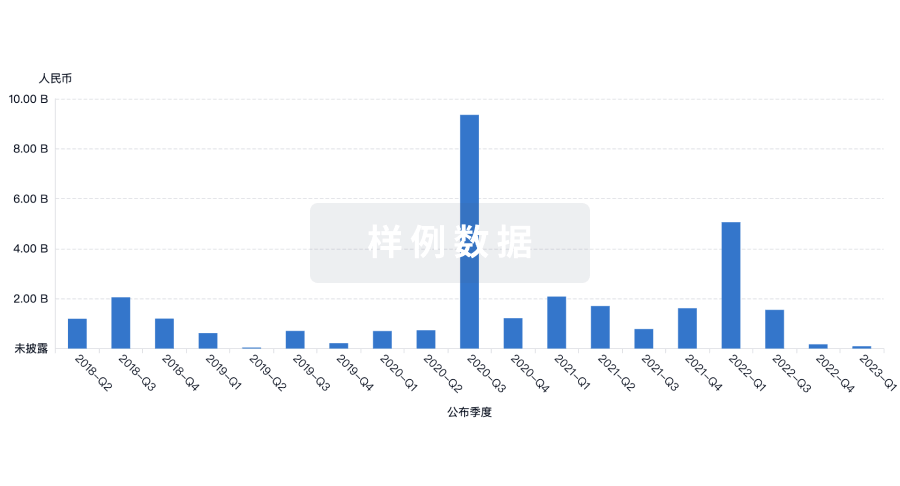
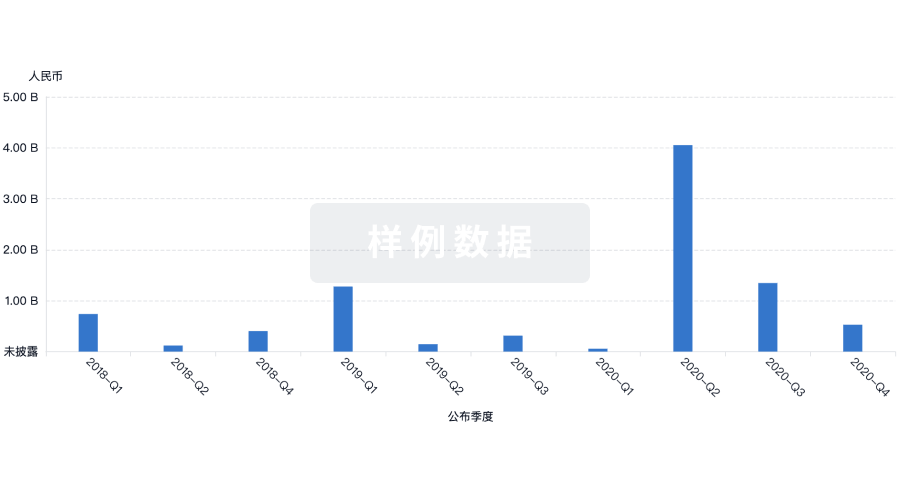
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用