预约演示
更新于:2025-08-29
Guardant Health, Inc.
更新于:2025-08-29
概览
关联
NCT07004413
Randomized Study to Compare First-line Treatment With Either Continuous or Intermittent Cetuximab Plus FOLFIRI in Patients With RAS/BRAF-wild-type Metastatic Colorectal Cancer (mCRC): AIO-KRK-0524 / FIRE-11
NCT06880055
Shield Post-Approval Study Protocol
JPRN-jRCT1050240085
MRD DETECTION AND LONGITUDINAL MONITORING OF MOLECULAR RECURRENCE USING GUARDANT REVEAL ASSAY IN LUNG CANCER PATIENTS WHO RECEIVE CURATIVE-INTENT LOCAL TREATMENTS
100 项与 Guardant Health, Inc. 相关的临床结果
登录后查看更多信息
登录后查看更多信息
2025-08-01EBioMedicine
A bedside-to-bench translational analysis of NF1 alterations and CDK4/6 inhibitor resistance in hormone receptor-positive metastatic breast cancer
Article
作者: Ma, Cynthia X ; Napolitano, Fabiana ; Liao, Jiemin ; Arteaga, Carlos L ; Liu, Shiyuan A ; Zhang, Nicole ; Chica-Parrado, Rosario ; Ye, Dan ; Uemoto, Yasuaki ; Wander, Seth A ; Bardia, Aditya ; Hanker, Ariella B ; Podany, Emily L ; Weipert, Caroline M ; Clifton, Katherine K ; Lin, Chang-Ching ; Keenan, Jennifer C ; Walko, Christine M ; Lloyd, Maxwell R ; Medford, Arielle J ; Ellisen, Leif W ; Wegrzyn, Claire ; Ryan, Lianne Y ; Knepper, Todd C ; Han, Hyo S ; Wulf, Gerburg M
BACKGROUND:
CDK4/6 inhibitors (CDK4/6i) are used for management of hormone receptor-positive (HR+) metastatic breast cancer (MBC), and activation of the RAS/MAPK and PI3K/AKT signalling pathways has been implicated in resistance to these agents. Pathogenic NF1 mutations (pNF1m) dysregulate RAS signalling, but NF1 has not been linked to CDK4/6i resistance. We analysed multi-institutional data, real-world evidence, and preclinical models to characterise the impact of pNF1m on CDK4/6i sensitivity.
METHODS:
A retrospective cohort of patients with pNF1m tumours were identified from 4 institutions between 2/2015-5/2023 and evaluated for progression-free survival and intrinsic/acquired resistance on CDK4/6i. Real-world clinical-genomic data from GuardantINFORM between 6/2014 and 3/2023 was analysed for associations between pNF1m and time-to-next-treatment or overall survival following CDK4/6i, adjusted using propensity score weighting. We used CRISPR/Cas9 to delete NF1 in MCF7 and T47D breast cancer cells in vitro. NF1-knockout (NF1-KO) and -wild-type (WT) cells were analysed with respect to CDK4/6i sensitivity, MAPK and PI3K pathway activation, and sensitivity to MAPK and PI3K pathway inhibitors. In parallel, we assessed treatment response in a patient-derived organoid (PDO) harbouring NF1 loss, established from an HR+/HER2- breast tumor following progression on a CDK4/6i.
FINDINGS:
Among 1962 multicentre patients, we identified 38 with HR+/HER2- MBC, pNF1m, and exposure to CDK4/6i. NF1-associated intrinsic or acquired resistance to CDK4/6i was observed in a majority of tumours, and in those with baseline pNF1m on first-line CDK4/6i, a median progression-free survival of 6.2 months was much less than expected in routine practice. Real-world weighted analysis of 1161 patients comparing 28 pNF1m to 1133 NF1 non-altered tumours demonstrated shorter time-to-next-treatment on CDK4/6i regimens (4.2 vs. 12.4 months, hazard ratio 3.14, 95% confidence interval 2.01-4.93) and overall survival (15.8 vs. 45.2 months, hazard ratio 2.04, 95% confidence interval 1.09-3.82). NF1-deleted cells exhibited reduced sensitivity to CDK4/6i with or without oestrogen suppression, which was accompanied by induction of both MAPK and PI3K pathways, the latter of which was exacerbated by CDK4/6i. Blockade of RAS or AKT, but not MEK or ERK, reversed CDK4/6i resistance mediated by NF1 loss in cell lines and the PDO.
INTERPRETATION:
NF1 mutations are associated with shorter therapy duration on CDK4/6i in MBC. A causal link between NF1 loss and CDK4/6i resistance was supported by experiments in HR + breast cancer cells. NF1 deletion was accompanied by activation of ERK and AKT, and blockade of RAS or AKT combined with CDK4/6i was effective in NF1-deleted cells and an NF1-mutant PDO.
FUNDING:
Breast Cancer Research Foundation DRC-20-001, National Cancer Institute R01CA273246, National Institute of Health P30 CA142543, Susan G. Komen Breast Cancer Foundation SAB1800010, Department of Defence BC 210406, Mary Kay Ash Foundation International Postdoctoral Scholars in Cancer Research Fellowship.
2025-07-01CANCER CELL
Induction of a mismatch repair deficient genotype by tailored chemical mutagenesis in experimental models of cancer
Article
作者: White, James R ; Johannet, Paul ; Vitiello, Pietro Paolo ; Patel, Mitesh ; Lu, Sydney ; Lu, Steve ; Segal, Neil H ; Zhang, Lin ; Artz, Oliver ; Shah, Rachna ; Gerber, Drew ; Monette, Sebastien ; Rangavajhula, Karthik ; Stephens, Dennis ; Rosiek, Eric ; Membreno-Berganza, Nathalie ; Weipert, Caroline M ; Lamendola-Essel, Michelle F ; Vlachos, Georgios ; Germano, Giovanni ; Abdel-Wahab, Omar ; Ma, Xiaoxiao ; Vidal, Joana ; Piastra-Facon, Florence ; de Stanchina, Elisa ; Cercek, Andrea ; Bardelli, Alberto ; Fidele, Deborah ; Kahn, Alec ; Randrian, Violaine ; Foote, Michael B ; Stewart, Caitlin M ; Mieles, David ; Abdelfattah, Somer ; Mehta, Shub ; Barlas, Afsar ; Bowker, Sydney ; Patel, Shrey ; Diaz, Luis A ; Bhattacharya, Rohini ; Hayatt, Omar ; Qu, Rui ; He, Bing ; Chan, Tim A ; Maron, Steven B ; Rousseau, Benoit ; Mandal, Rajarsi ; Argilés, Guillem ; Luo, Lingqi ; Zhang, Taotao
Mismatch repair deficient (MMRd) tumors harbor thousands of somatic mutations enriched for insertion-deletion (indels) conferring high sensitivity to immunotherapy. We sought to reproduce this phenotype using mutagenic agents to engineer an MMRd genotype in immunoresistant cells. The combination of temozolomide (TMZ) and cisplatin led to a rapid accumulation of a high mutational load enriched for indels in murine cell lines resulting from the epigenetic loss of Msh2. Pretreated cells showed sensitivity to PD-1 blockade. Systemic treatment with TMZ, cisplatin, and anti-PD-1 bearing immunoresistant tumor cells led to increased survival, intratumoral T cell infiltration, and downregulation of Msh2 expression without affecting healthy tissues. In a clinical trial with 18 patients with refractory mismatch repair proficient colorectal cancer, no responses were seen, but MMRd signatures emerged in cell-free DNA. These findings show that recapitulating an MMRd genotype through chemical mutagenesis can generate an immunogenic phenotype.
2025-07-01GASTROENTEROLOGY
Colonoscopic Follow-Up After Abnormal Blood-Based Colorectal Cancer Screening Results
Article
作者: Raymond, Victoria M ; May, Folasade P ; Zaki, Timothy A ; Zhang, Nicole J ; Das, Amar K ; Forbes, Shaun P
2025-08-26
·循因缉药
并购信使RNA临床研究
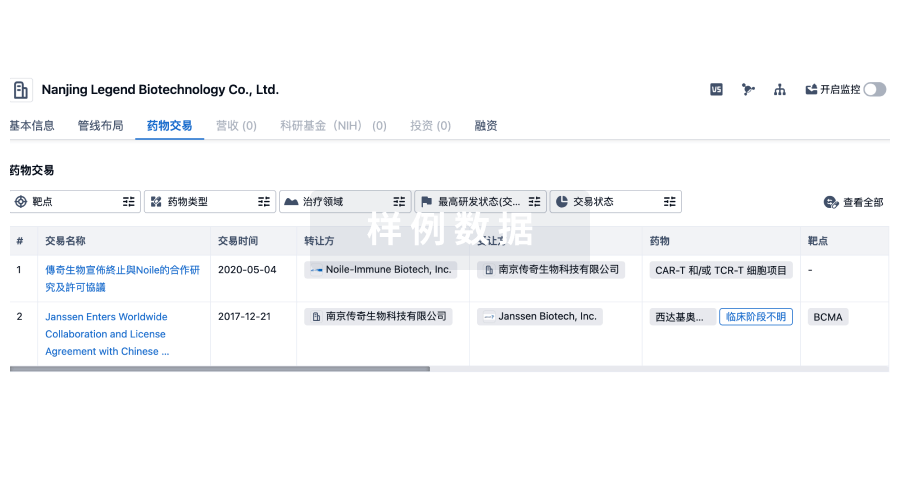
100 项与 Guardant Health, Inc. 相关的药物交易
登录后查看更多信息
100 项与 Guardant Health, Inc. 相关的转化医学
登录后查看更多信息
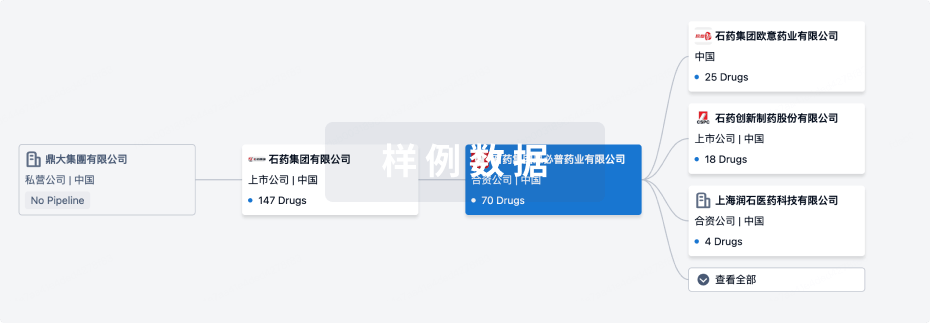
组织架构
使用我们的机构树数据加速您的研究。
登录
或
管线布局
2025年08月30日管线快照
无数据报导
登录后保持更新
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
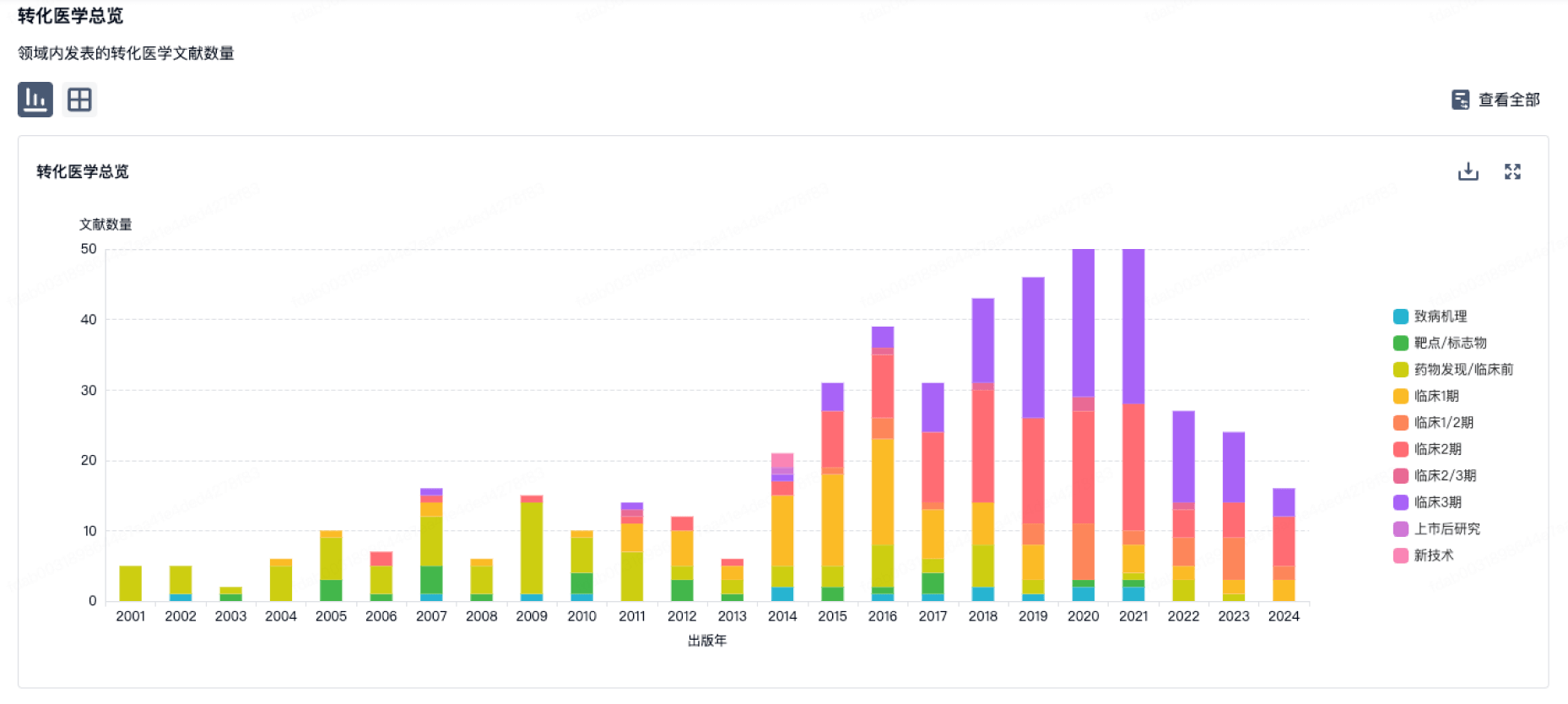
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
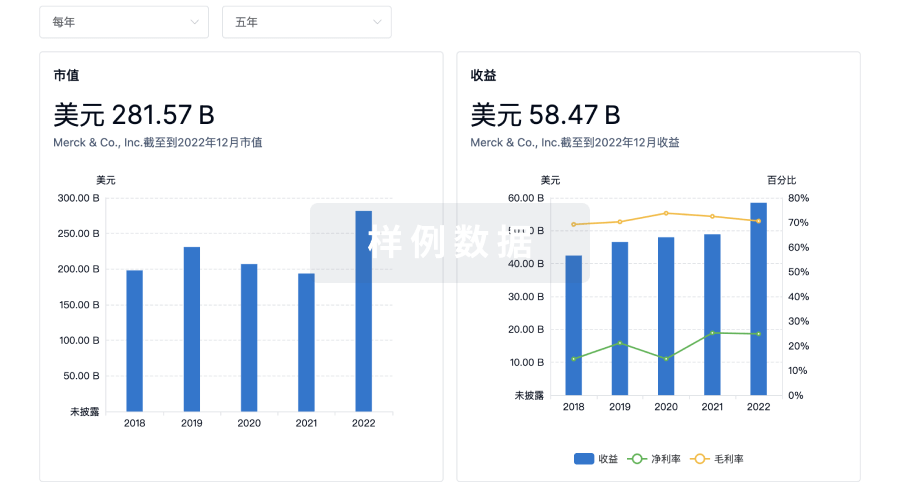
营收
使用 Synapse 探索超过 36 万个组织的财务状况。
登录
或
科研基金(NIH)
访问超过 200 万项资助和基金信息,以提升您的研究之旅。
登录
或

投资
深入了解从初创企业到成熟企业的最新公司投资动态。
登录
或
融资
发掘融资趋势以验证和推进您的投资机会。
登录
或
Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用