更新于:2024-12-05
STX-300s
更新于:2024-12-05
概要
基本信息
原研机构 |
在研机构 |
非在研机构- |
最高研发阶段药物发现 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |
关联
100 项与 STX-300s 相关的临床结果
登录后查看更多信息
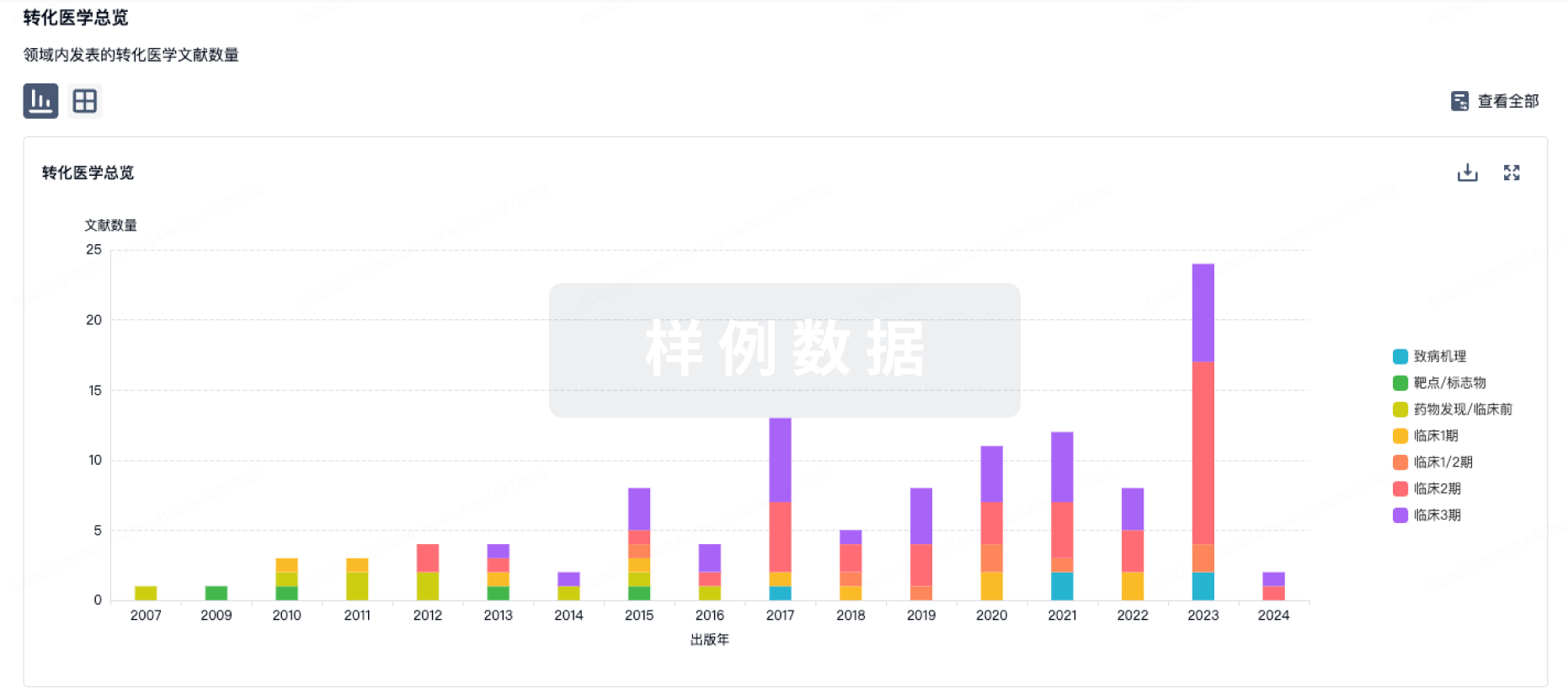
100 项与 STX-300s 相关的转化医学
登录后查看更多信息
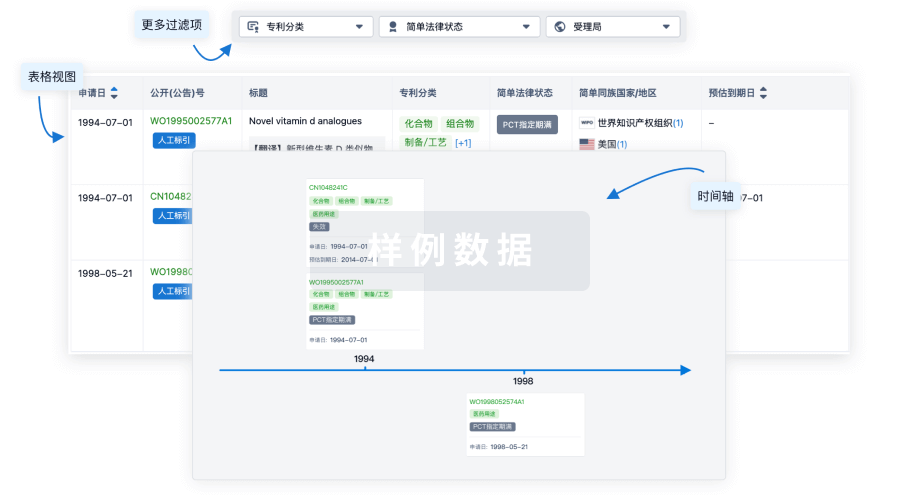
100 项与 STX-300s 相关的专利(医药)
登录后查看更多信息
13
项与 STX-300s 相关的文献(医药)2024-11-01·DRUGS
Slowing the Progression of Chronic Kidney Disease in Patients with Type 2 Diabetes Using Four Pillars of Therapy: The Time to Act is Now
Review
作者: Koufakis, Theocharis ; Georgianos, Panagiotis I ; Vaios, Vasilios ; Liakopoulos, Vassilios
Chronic kidney disease (CKD) is the most common co-morbidity in patients with type 2 diabetes (T2D) and its presence substantially amplifies the risk for premature death, adverse cardiovascular events, and faster progression of kidney injury to kidney failure. For nearly two decades, the pharmacological blockade of the renin-angiotensin-system (RAS) was the only pillar of therapy to afford cardiorenal protection in these patients. During the last 5 years, newer novel therapies have been added to our therapeutic armamentarium, offering promise for more effective management of diabetic kidney disease in the future. Large phase 3 clinical trials have demonstrated additive cardiorenal protective benefits of sodium-glucose co-transporter type 2 (SGLT-2) inhibitors, the non-steroidal mineralocorticoid-receptor-antagonist (MRA) finerenone, and glucagon-like peptide-1 receptor agonist (GLP-1RA) semaglutide relative to placebo in patients with albuminuric CKD and T2D who are receiving standard-of-care treatment with a RAS-blocker. These therapies are likely much more effective when administered in a combined therapeutic algorithm, but the potential additive effects of combination therapy remain to be established in ongoing clinical trials. In this article, we assemble four pillars of therapy for the attenuation of residual cardiorenal risk in patients with CKD associated with T2D. We provide evidence from recent randomized trials and we discuss the concept of combined treatment for maximal cardiorenal protection in this high-risk patient population.
2021-04-08·Current pharmaceutical design4区 · 医学
Mechanisms for Cardiorenal Protection of SGLT-2 Inhibitors
4区 · 医学
Article
作者: Salmas, Marios ; Georgianos, Panagiotis I. ; Liakopoulos, Vassilios ; Dounousi, Evangelia ; Vaios, Vasilios ; Eleftheriadis, Theodoros
Despite optimal treatment of diabetic kidney disease (DKD) with adequate blood pressure control
and agents blocking the renin-angiotensin-system (RAS), the residual cardiorenal risk of these patients remains
substantially high. There is, therefore, an unmet need for additional therapies effective to retard the progression
of DKD and improve cardiovascular outcomes in this high-risk population. Sodium-glucose co-transporter 2
(SGLT-2) inhibitors represent a novel drug class that received regulatory approval for improving glycemic control
in patients with type 2 diabetes and preserved kidney function. Large outcome trials designed to test their
cardiovascular safety profile showed an unexpected improvement in cardiovascular outcomes and also suggested
a slower progression of DKD with SGLT-2 inhibition. The Canagliflozin and Renal Outcomes in Type 2 Diabetes
and Nephropathy (CREDENCE), a trial that was designed to specifically investigate the renoprotective
properties of SGLT-2 inhibitors in patients with overt DKD already receiving guideline-based therapy with a
RAS-blocker, was prematurely terminated due to an impressive benefit of canagliflozin on kidney and cardiovascular
outcomes. These impressive results refine the role and the indication of SGLT-2 inhibitors as a cardioand
renoprotective strategy in patients with DKD. In this article, we provide an overview of the available clinical-
trial evidence and explore the mechanisms mediating the cardiorenal protection afforded by SGLT-2 inhibitors.
We conclude with perspectives for a potential beneficial effect of this novel drug class in patients with
non-diabetic kidney disease.
2021-01-01·Journal of hypertension2区 · 医学
The corona-virus disease 2019 pandemic compromised routine care for hypertension: a survey conducted among excellence centers of the European Society of Hypertension
2区 · 医学
Article
作者: J Redon ; C Rajkumar ; Wks Barroso ; Y Sirenko ; A Oliveras ; J Vaclavik ; E Nasr ; Gs Stergiou ; Z Gaciong ; D Raev ; R Pontremoli ; Nr Robles ; M Viigimaa ; M Volpe ; A Mazza ; M Glover ; Stojanov ; R Kreutz ; Tk Makris ; P Zebekakis ; Z Jarai ; M Okorie ; I Barna ; S Obregon ; T De Backer ; R Sarzani ; F Mallamaci ; M Marketou ; R Zweiker ; M Azizi ; A Januszewicz ; Ea Rosei ; Es Muxfeldt ; M Dorobantu ; G Abraham ; C Giannattasio ; Lc Rump ; F Veglio ; C Grassos ; Z Parounak ; Aj Manolis ; I Tikkanen ; E Lurbe ; K Tsioufis ; Ml Muiesan ; C Sierra ; S Eckert ; D Webb ; T Weber ; Fj Aguila ; Weber, Thomas ; A Gottsater ; Jd Mediavilla ; T Kahan ; I Papadakis ; D Lovic ; J Brguljan ; M Lopez-Sublet ; N Chapman
Background::
The Covid-19 pandemic caused a shutdown of healthcare systems in many countries. We explored the impact on hypertension care in the Excellence Center (EC) network of the European Society of Hypertension.
Methods::
We conducted a 17-question electronic survey among ECs.
Results::
Overall, 52 ECs from 20 European and three non-European countries participated, providing hypertension service for a median of 1500 hypertensive patients per center per year. Eighty-five percent of the ECs reported a shutdown lasting for 9 weeks (range 0–16). The number of patients treated per week decreased by 90%: from a median of 50 (range 10–400) before the pandemic to a median of 5.0 (range 0–150) during the pandemic (P < 0.0001). 60% of patients (range 0–100%) declared limited access to medical consultations. The majority of ECs (57%) could not provide 24-h ambulatory BP monitoring, whereas a median of 63% (range 0–100%) of the patients were regularly performing home BP monitoring. In the majority (75%) of the ECs, hypertension service returned to normal after the first wave of the pandemic. In 66% of the ECs, the physicians received many questions regarding the use of renin–angiotensin system (RAS) blockers. Stopping RAS-blocker therapy (in a few patients) either by patients or physicians was reported in 27 and 36.5% of the ECs.
Conclusion::
Patient care in hypertension ECs was compromised during the Covid-19-related shutdown. These data highlight the necessity to develop new strategies for hypertension care including virtual clinics to maintain services during challenging times.
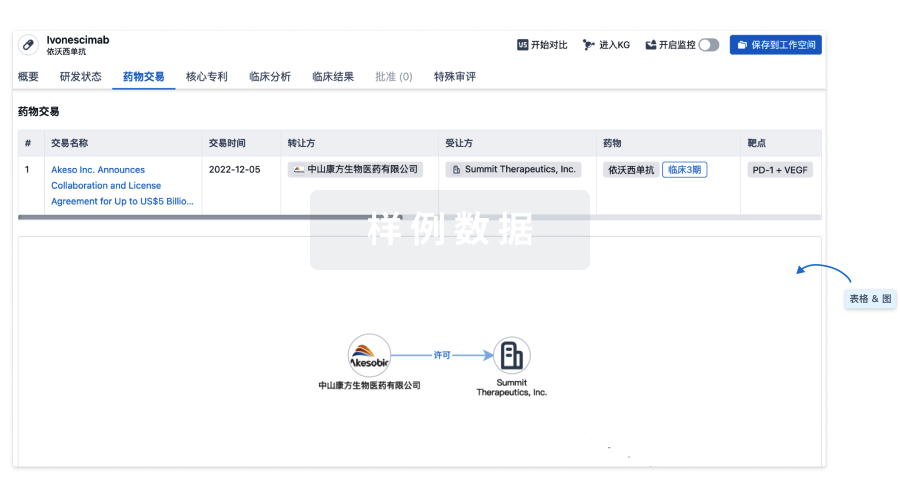
100 项与 STX-300s 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 肿瘤 | 药物发现 | 美国 | 2022-01-30 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
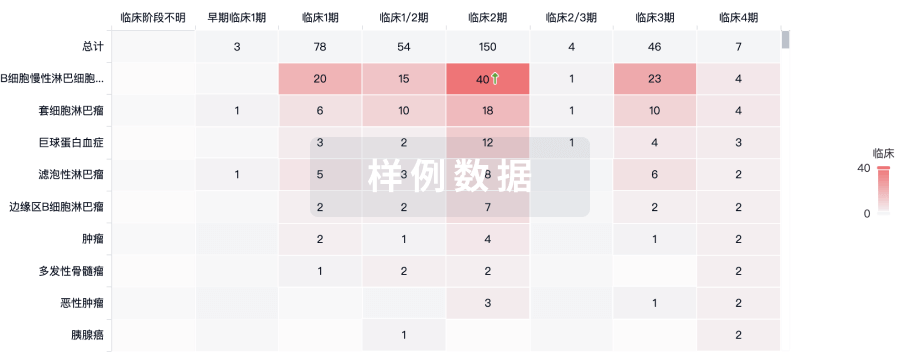
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

标准版
¥16800
元/账号/年
新药情报库 | 省钱又好用!
立即使用
来和芽仔聊天吧
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用