预约演示
更新于:2024-12-26
GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium)
更新于:2024-12-26
概要
基本信息
非在研机构- |
最高研发阶段临床1期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |
登录后查看时间轴
关联
1
项与 GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium) 相关的临床试验NCT02149225
A Phase I Trial of Actively Personalized Peptide Vaccinations Plus Immunomodulators in Patients With Newly Diagnosed Glioblastoma Concurrent to First Line Temozolomide Maintenance Therapy
100 项与 GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium) 相关的临床结果
登录后查看更多信息
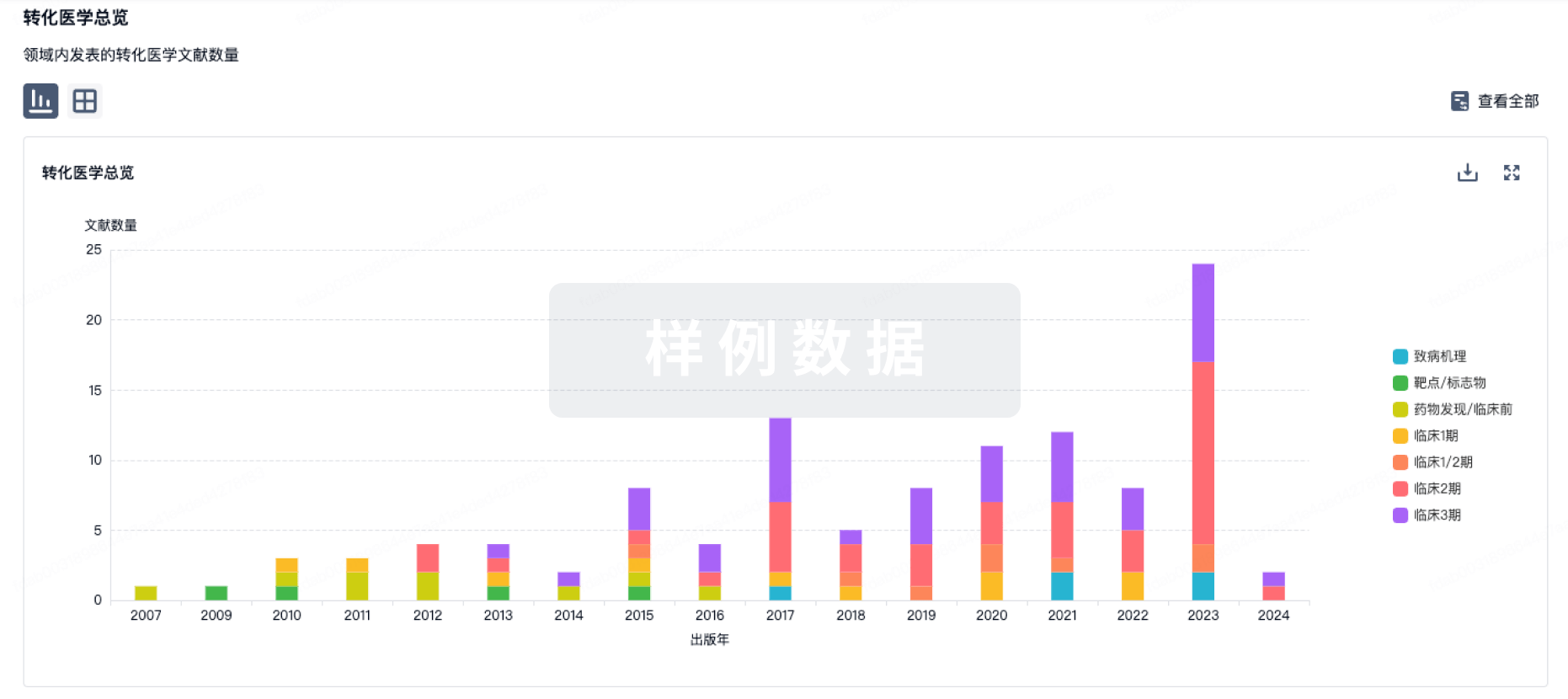
100 项与 GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium) 相关的转化医学
登录后查看更多信息
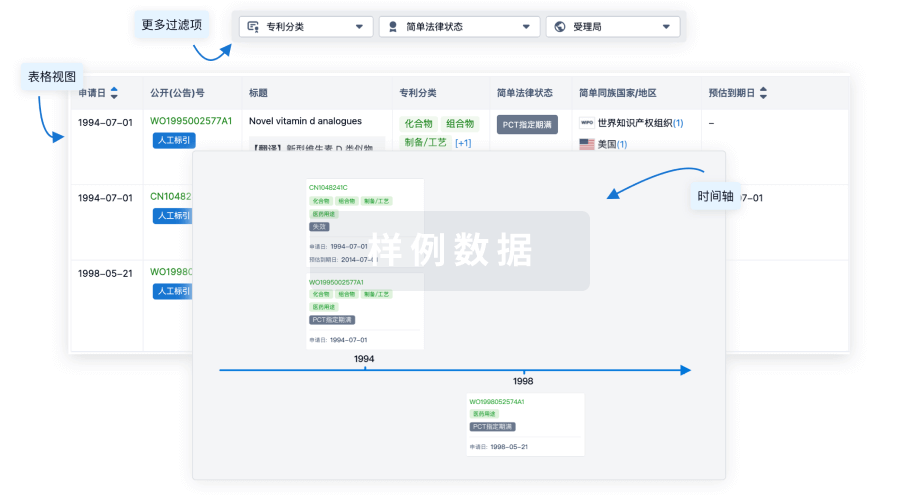
100 项与 GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium) 相关的专利(医药)
登录后查看更多信息
3
项与 GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium) 相关的文献(医药)2019-01-10Nature
Actively personalized vaccination trial for newly diagnosed glioblastoma
Article
作者: Green, Edward ; Derhovanessian, Evelyna ; von Deimling, Andreas ; Ulges, Alexander ; Okada, Hideho ; Gouttefangeas, Cécile ; Kroep, Judith R ; Ponsati, Berta ; Singh-Jasuja, Harpreet ; Shraibman, Bracha ; Reinhardt, Carsten ; Huber, Christoph ; Kiesel, Katharina ; Migliorini, Denis ; Bukur, Valesca ; Sahuquillo, Juan ; Hoffgaard, Franziska ; Wick, Wolfgang ; Lassen, Ulrik ; Stevanović, Stefan ; Castle, John C ; Kemmer-Brück, Alexandra ; Dorner, Sonja ; Dietrich, Pierre-Yves ; Ottensmeier, Christian H ; Sahin, Ugur ; van der Burg, Sjoerd H ; Capper, David ; Tabatabai, Ghazaleh ; Britten, Cedrik M ; Kreiter, Sebastian ; Tadmor, Arbel D ; Dutoit, Valerie ; Admon, Arie ; Poulsen, Hans S ; Rusch, Elisa ; Rammensee, Hans-Georg ; Heesch, Sandra ; Fritsche, Jens ; Platten, Michael ; Piró, Jordi ; Bunse, Lukas ; Song, Colette ; Martínez-Ricarte, Francisco ; Hilf, Norbert ; Skardelly, Marco ; Frenzel, Katrin ; Stieglbauer, Monika ; Idorn, Manja ; Ludwig, Jörg ; Thor Straten, Per ; Welters, Marij J P ; McCann, Katy ; Maurer, Dominik ; Mendrzyk, Regina ; Meyer, Miriam ; Kuttruff-Coqui, Sabrina ; Rössler, Bernhard ; Rodon, Jordi ; Wagner, Claudia ; Weinschenk, Toni ; Schoor, Oliver ; Löwer, Martin ; Pawlowski, Nina
Patients with glioblastoma currently do not sufficiently benefit from recent breakthroughs in cancer treatment that use checkpoint inhibitors1,2. For treatments using checkpoint inhibitors to be successful, a high mutational load and responses to neoepitopes are thought to be essential3. There is limited intratumoural infiltration of immune cells4 in glioblastoma and these tumours contain only 30-50 non-synonymous mutations5. Exploitation of the full repertoire of tumour antigens-that is, both unmutated antigens and neoepitopes-may offer more effective immunotherapies, especially for tumours with a low mutational load. Here, in the phase I trial GAPVAC-101 of the Glioma Actively Personalized Vaccine Consortium (GAPVAC), we integrated highly individualized vaccinations with both types of tumour antigens into standard care to optimally exploit the limited target space for patients with newly diagnosed glioblastoma. Fifteen patients with glioblastomas positive for human leukocyte antigen (HLA)-A*02:01 or HLA-A*24:02 were treated with a vaccine (APVAC1) derived from a premanufactured library of unmutated antigens followed by treatment with APVAC2, which preferentially targeted neoepitopes. Personalization was based on mutations and analyses of the transcriptomes and immunopeptidomes of the individual tumours. The GAPVAC approach was feasible and vaccines that had poly-ICLC (polyriboinosinic-polyribocytidylic acid-poly-L-lysine carboxymethylcellulose) and granulocyte-macrophage colony-stimulating factor as adjuvants displayed favourable safety and strong immunogenicity. Unmutated APVAC1 antigens elicited sustained responses of central memory CD8+ T cells. APVAC2 induced predominantly CD4+ T cell responses of T helper 1 type against predicted neoepitopes.
OncoTargets and therapy4区 · 医学
<p>A Hybrid Glioma Tumor Cell Lysate Immunotherapy Vaccine Demonstrates Good Clinical Efficacy in the Rat Model</p>
4区 · 医学
ArticleOA
作者: Chen, Li-Gang ; Peng, Li-Lei ; Zeng, Shan ; He, Hai-Ping ; Zeng, Xu ; Li, Xin-Long
BACKGROUND:
Conventional immunotherapy for glioma is not only expensive but also demonstrates less-than-desired clinical efficacy. In this study, we evaluated the immunotherapeutic efficacy of a tumor cell lysate-based hybrid glioma vaccine developed using a molecular-based approach.
METHODS:
First, the ability of the autologous (9L-cell lysate) and allogeneic (C6-cell lysate) vaccines against glioma, individually and in combination, to activate Fischer344 rat dendritic cells (DCs) was determined. Next, the activated DCs were co-cultured with T lymphocytes and screened for the optimal DC-to-T-cell ratio. The in vitro efficacy of the DC/T-cell vaccine formulations subjected to different immunogen treatments and co-cultured with glioma cells was evaluated based on glioma cell viability and monocyte chemoattractant protein (MCP)-2 and interferon (IFN)-γ secretion. Subsequently, the efficacy of the 9L + C6 hybrid vaccine was evaluated in 32 glioma rat models, randomly allocated to the following five treatment groups: blank control, tumor, vaccine treatment, thymosin treatment, and vaccine + thymosin treatment (combined treatment). Changes in survival duration, intracranial tumor volume, peripheral blood immune-cell (CD4+ T, CD8+ T, and natural killer [NK] cell) count, and serum cytokine (interleukin [IL]-2, IL-10) levels were assessed in these groups.
RESULTS:
The hybrid vaccine demonstrated the highest glioma cell apoptosis and the lowest cell viability and promoted MCP-2 and IFN-γ secretion in vitro. The vaccine treatment and combined treatment groups demonstrated longer survival duration, lower intracranial tumor volume, and higher immune cell glioma tissue infiltration and IL-2 secretion than the untreated tumor group, indicating the vaccine's good in vivo efficacy. Thymosin treatment had minimal effect in enhancing anti-glioma immunity.
CONCLUSION:
We demonstrated the feasibility of combining autologous and allogeneic tumor cell lysates to stimulate specific host cell immune response against glioma cells. The good clinical efficacy of our developed glioma hybrid vaccine in rat models suggests its potential clinical application.
International journal of general medicine4区 · 医学
Efficacy and Safety of Actively Personalized Neoantigen Vaccination in the Management of Newly Diagnosed Glioblastoma: A Systematic Review
4区 · 医学
ReviewOA
作者: Li, Zihuang ; Yang, Hongli ; Khan, Muhammad ; Liao, Guixiang ; Yan, Maosheng ; Li, Xianming
PURPOSE:
Glioblastoma (GBM) shows frequent relapse and is highly resistant to treatment; therefore, it is considered fatal. Various vaccination protocols that have been tested in patients with GBM, which is the most common and aggressive primary brain tumor, have indicated safety and efficacy, to some extent, when used alone or in combination with standard of care. Recently, neoantigen-based personalized vaccines have shown tremendous immunogenicity and safety in GBM. We aimed to systematically review the medical literature for clinical trials to evaluate the efficacy and safety of neoantigen-based personalized vaccines for newly diagnosed GBM.
METHODS:
We conducted a literature search for clinical trials on PubMed, Cochrane Library, China National Knowledge Infrastructure, and ClinicalTrials.gov until March 20, 2021. The primary outcomes of interest were immunogenicity and safety of the therapy. Efficacy outcomes, such as progression-free survival and overall survival, were secondary outcomes of interest.
RESULTS:
Two clinical trials involving 24 patients were included in this review. High immunogenicity was observed in both studies. The GAPVAC-101 trial reported 50% APVAC1-induced and 84.7% APVAC2-induced immunogenicity with CD8+ and CD4+ T cell responses in 92% (12/13) and 80% (8/10) immune responders, respectively. Two out of five patients showed CD4+ and CD8+ T cell responses in the study by Keskin et al. Dexamethasone use had limited immunogenicity in a trial by Keskin et al (6/8). No serious treatment-related adverse events were reported.
CONCLUSION:
Actively personalized vaccines aimed at unmutated peptides and neoantigens for patients with GBM are safe and highly immunogenic, particularly when administered in combination. Larger studies are warranted to investigate the role.
1
项与 GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium) 相关的新闻(医药)2022-06-19
疫苗信使RNA免疫疗法抗体基因疗法
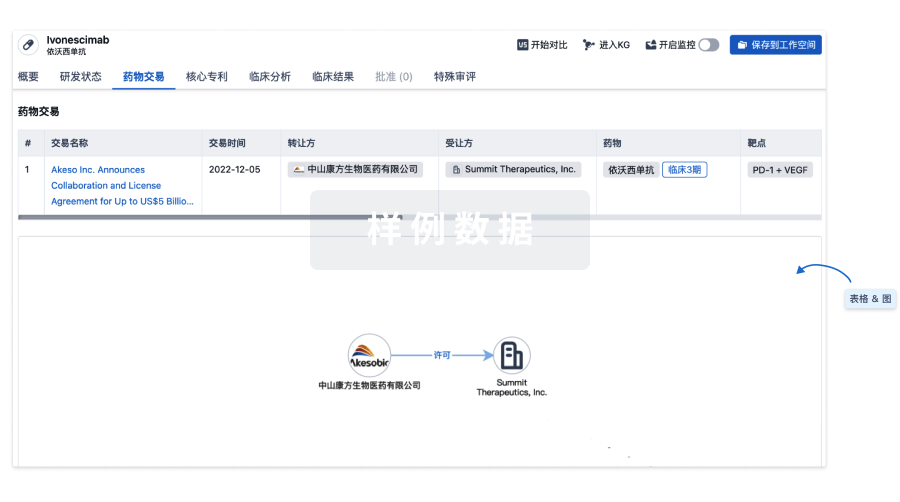
100 项与 GliomaGlioblas peptide vaccine(Glioma Actively Personalized Vaccine Consortium) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 胶质母细胞瘤 | 临床2期 | 瑞士 | 2014-09-30 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
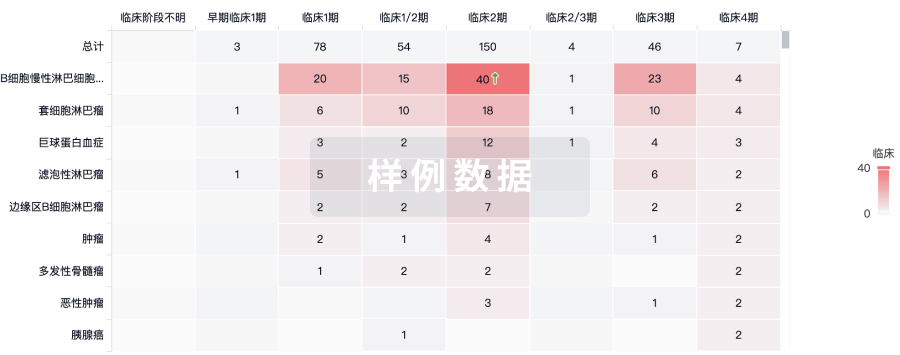
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

来和芽仔聊天吧
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用