预约演示
更新于:2025-08-16
Anti-CD19 CAR T-cell therapy (Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences )
更新于:2025-08-16
概要
基本信息
药物类型 CAR-T |
别名- |
靶点 |
作用方式 抑制剂 |
作用机制 CD19抑制剂(B淋巴细胞抗原CD19抑制剂) |
在研适应症 |
非在研机构- |
权益机构- |
最高研发阶段临床2期 |
首次获批日期- |
最高研发阶段(中国)临床2期 |
特殊审评- |
登录后查看时间轴
关联
5
项与 Anti-CD19 CAR T-cell therapy (Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences ) 相关的临床试验NCT06680388
Exploratory Clinical Study to Evaluate the Safety and Efficacy of Autologous CD19 CAR-T in the Treatment of Relapsed/Refractory Autoimmune Diseases
Autoimmune diseases such as systemic lupus erythematosus (SLE), diffuse cutaneous systemic sclerosis (dcSSc), antineutrophil cytoplasmic antibody (ANCA) -associated vasculitis (AAV), idiopathic inflammatory myopathy (IIM), and Sjogren's syndrome (SS) have complex etiologies and are prone to cause systemic multiple organ damage. Because patients need lifelong medication due to repeated disease recurrence, and the current treatment of the above autoimmune diseases has limited efficacy and greater side effects, so that patients bear an excessive burden of disease, therefore, there is an urgent need to explore safer and more effective treatment.
Several autologous CAR-T products targeting CD19 have been marketed for the treatment of B-cell hematological malignancies. Depletion of B cells to suppress abnormal immune responses is also currently one of the popular strategies for the treatment of antibody-mediated autoimmune diseases, and many clinical studies of CAR-T against autoimmune diseases are still ongoing.
Therefore, a dose escalation trial is planned to evaluate the safety, tolerability, and preliminary efficacy of autologous CD19 CAR-T in patients with relapsed/refractory autoimmune diseases.
Several autologous CAR-T products targeting CD19 have been marketed for the treatment of B-cell hematological malignancies. Depletion of B cells to suppress abnormal immune responses is also currently one of the popular strategies for the treatment of antibody-mediated autoimmune diseases, and many clinical studies of CAR-T against autoimmune diseases are still ongoing.
Therefore, a dose escalation trial is planned to evaluate the safety, tolerability, and preliminary efficacy of autologous CD19 CAR-T in patients with relapsed/refractory autoimmune diseases.
开始日期2024-11-15 |
申办/合作机构- |
NCT06608342
Clinical Study of Autologous Hematopoietic Stem Cell Transplantation Combined With CD19-CART Treatment for Adult High-risk Acute Lymphoblastic Leukemia
To observe the efficacy and side effects of autologous hematopoietic stem cell transplantation combined with CD19-CART for adult acute lymphoblastic leukemia, and to evaluate the safety and efficacy of this regimen in the treatment of acute lymphoblastic leukemia.
开始日期2024-06-25 |
申办/合作机构 中国医学科学院血液病医院 [+1] |
NCT06464185
A Prospective Clinical Study of CD3-CD20 Bisspecific Antibody Based Therapy Combined With CD19-CAR T Cells in the Treatment of Relapsed Refractory B-cell Non-Hodgkin Lymphoma
The aim of this study was to analyze the safety and efficacy of CD3-CD20 bispecific antibody-based therapy in combination with CD19-CAR-T cells for the treatment of relapsed and refractory B-cell Non-Hodgkin's (B-NHL) lymphoma.
The main questions it aims to answer:
1. The safety of CD3-CD20 bispecific antibody-based therapy in combination with CD19-CAR-T cells in B-NHL;
2. The effect of different doses of bispecific antibody maintenance therapy on CAR-T cell expansion.
The main questions it aims to answer:
1. The safety of CD3-CD20 bispecific antibody-based therapy in combination with CD19-CAR-T cells in B-NHL;
2. The effect of different doses of bispecific antibody maintenance therapy on CAR-T cell expansion.
开始日期2024-04-30 |
申办/合作机构 |
100 项与 Anti-CD19 CAR T-cell therapy (Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences ) 相关的临床结果
登录后查看更多信息
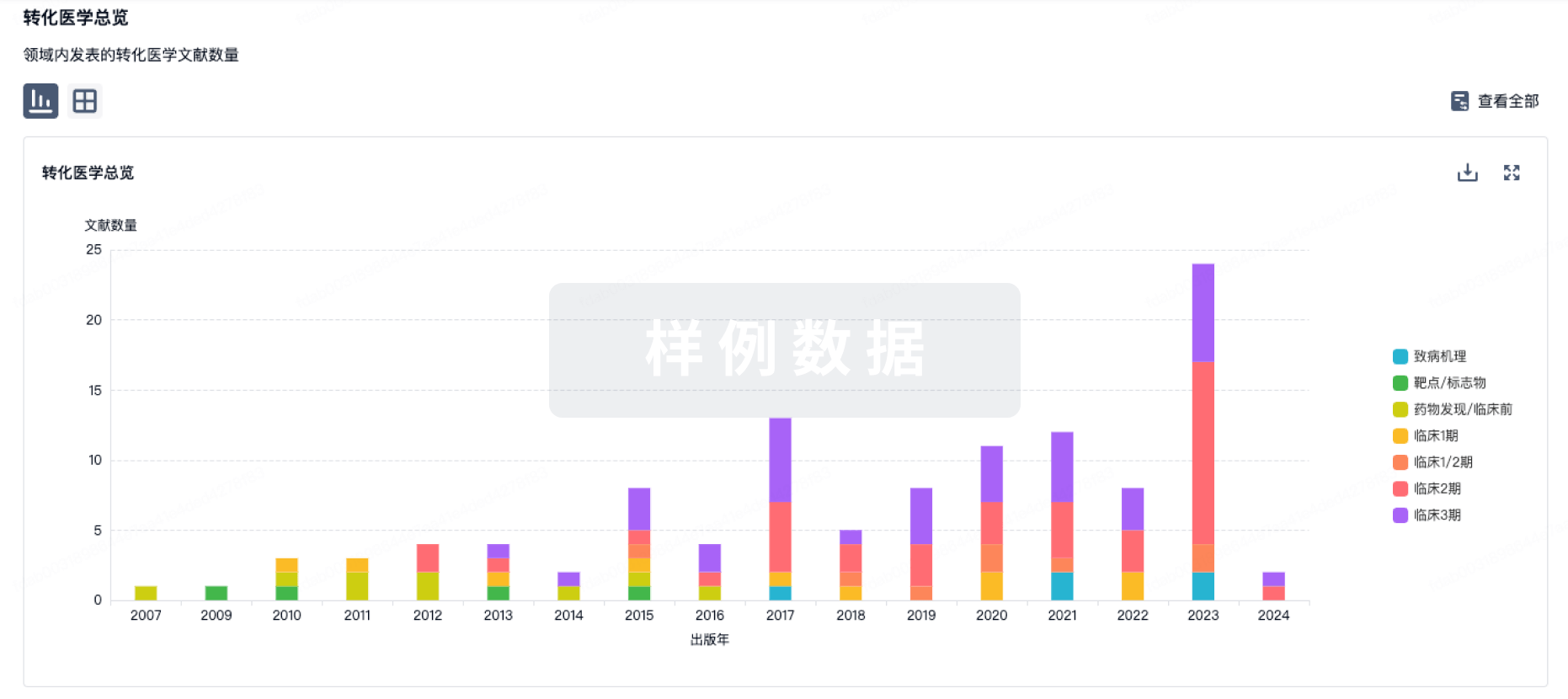
100 项与 Anti-CD19 CAR T-cell therapy (Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences ) 相关的转化医学
登录后查看更多信息
100 项与 Anti-CD19 CAR T-cell therapy (Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences ) 相关的专利(医药)
登录后查看更多信息
3
项与 Anti-CD19 CAR T-cell therapy (Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences ) 相关的新闻(医药)2024-06-20
Drs. Marko Radic and Georg Schett Honored at FOCIS 2024 Meeting
SAN FRANCISCO, June 20, 2024 /PRNewswire/ -- The Lupus Research Alliance (LRA) announced the recipients of the 2024 Lupus Insight Prize to Marko Radic, Ph.D., The University of Tennessee Health Science Center, and Georg Schett, M.D., Friedrich-Alexander-Universität Erlangen-Nürnberg, for their groundbreaking discoveries in utilizing CAR T cell therapy to potentially revolutionize lupus treatment. Drs. Radic and Schett were honored at a celebratory award ceremony during the Federation of Clinical Immunology Societies (FOCIS) 2024 meeting.
Continue Reading
Drs. Marko Radic and Georg Schett receiving the Lupus Research Alliance 2024 Lupus Insight Prize
The Lupus Insight Prize is awarded to outstanding investigators who have made a significant discovery in the last five years that will advance our understanding of the development, diagnosis, or treatment of lupus.
Revolutionizing Lupus Treatment Through CAR T Cell Therapy
T cells are an essential pillar of the immune system— they mount a response against harmful invaders, targeting and eliminating pathogens like viruses and bacteria to protect us from infection. Chimeric antigen receptor (CAR) T cell therapy involves reprogramming a patient's own T cells to target and eliminate cells contributing to the disease. CAR T cell therapy has garnered significant attention and success in cancer treatment. Drs. Marko Radic and Georg Schett have made pioneering contributions to the field of CAR T cell therapies for lupus, charting a new course in the treatment landscape and offering hope for individuals with this complex condition.
"We are thrilled to award Drs. Marko Radic and Georg Schett the 2024 Lupus Insight Prize for their groundbreaking contributions to engineered cell therapies in lupus," noted Teodora Staeva, Ph.D., Vice President and Chief Scientific Officer at the LRA. "Their innovative application of CAR T cell therapy offers unprecedented hope for a cure for individuals living with lupus."
Pioneering CAR T Cell Therapy in Mouse Models of Lupus
Dr. Marko Radic's seminal study, partly funded by the LRA, highlighted the profound efficacy of CAR T cells targeting CD19, a protein found on B cells. By using CD19-targeted CAR T cells to deplete B cells, which serve as key orchestrators of lupus disease, Dr. Radic's innovative approach reduced disease progression in two mouse models of lupus. The CAR T-treated mice lived longer, and several features of lupus were eliminated or reduced substantially, including autoantibodies, proteinuria (excess protein in the urine), and markers of inflammation. Notably, the CAR T cells continued working several months after administration. Dr. Radic's work laid the cornerstone for exploring CAR T cell therapy as a promising avenue for treating lupus in human patients, offering a glimpse into the potential of immunotherapy for autoimmune diseases.
Dr. Radic will use his Lupus Insight Prize to study how a process called trogocytosis affects the success or failure of CAR T cell therapy. In some cases, when a CAR T cell attaches to its target antigen (CD19 on the surface of B cells, in this case), the CAR T cell can take in a piece of the target cell's membrane, including CD19, without killing the target B cell. This process, called trogocytosis (also known as "cell nibbling"), may lead to exhaustion and death of the CAR T cells, potentially impacting the effectiveness of CAR T therapy. Dr. Radic's proposed study will guide the development of more effective cell therapies for people with lupus.
Translating CAR T Cell Therapy to Clinical Success
Building upon Dr. Radic's foundational research, Dr. Georg Schett made significant strides in translating CAR T cell therapy from preclinical studies to clinical application. In his groundbreaking publication and follow-up study, Dr. Schett and his team reported compelling outcomes from a single patient followed by a small case series involving individuals with refractory (resistant to treatment) lupus. Infusing CAR T cells that target CD19 eliminated B cells from the blood by the second day after CAR T administration. All individuals treated with anti-CD19 CAR T cells showed a reduction in or disappearance of lupus features including the presence of autoantibodies, nephritis (kidney inflammation), and other manifestations such as arthritis, fatigue, and lung issues.
In addition, four of the five patients reached a SLEDAI score (a commonly used tool to measure disease activity) of 0, indicating no detectable disease activity, and all five were able to stop taking immunosuppressive drugs, achieving drug-free remission. Notably, although their B cells returned about 100 days after CAR T cell therapy, lupus remained absent, raising the possibility that the immune system has been "rebooted" by the treatment, offering hope for transformative treatments for people with lupus who are resistant to conventional therapies.
CAR T cell administration effectively eliminated B cells from the individuals' blood. However, if some self-reactive B cells remain in the body's tissues, such as the lymph nodes, the immune system may continue to malfunction. Dr. Schett has recently developed a method to take tissue biopsies from people with lupus to assess the extent of B cell depletion in their lymph nodes, which are small lumps of tissue that are critical components of the immune system. He will use his Lupus Insight Prize to analyze these biopsies to assess how well the CD19-CAR T cell therapy was able to eliminate B cells from this tissue. These findings could inform and optimize treatment strategies, leading to improved long-term disease management and better patient outcomes.
The groundbreaking use of CAR T cell therapy represents a convergence of cutting-edge science and clinical innovation, signaling a major shift in our approach to lupus management. As we celebrate the remarkable achievements of both Drs. Radic and Schett, we eagerly anticipate the continued advancements that will emerge to unravel the complexities of lupus and improve outcomes for people with lupus.
About Lupus
Lupus is a chronic, complex autoimmune disease that affects millions of people worldwide. More than 90 percent of people with lupus are women, often striking during the childbearing years of 15-45. Black, Hispanic, Indigenous, and Asian/Pacific Islander people are disproportionately affected by lupus and are more likely to experience severe lupus symptoms. Black, Hispanic, Indigenous, and Asian/Pacific Islander people are disproportionately affected by lupus and are more likely to experience severe lupus symptoms. In lupus, the immune system, meant to defend against infections, produces antibodies that mistakenly recognize the body's own cells as foreign, prompting other immune cells to attack and potentially damage organs such as the kidneys, brain, heart, lungs, blood, skin, and joints.
About the Lupus Research Alliance
The Lupus Research Alliance is the largest non-governmental, non-profit funder of lupus research worldwide. The organization aims to transform treatment by funding the most innovative lupus research, fostering diverse scientific talent, and driving discovery toward better diagnostics, improved treatments, and ultimately, a cure for lupus. Because the Lupus Research Alliance's Board of Directors funds all administrative and fundraising costs, 100% of all donations goes to support lupus research programs. For more information, please visit the LRA at LupusResearch.org and on social media at:
X, Facebook, LinkedIn, and Instagram.
CONTACT:
Margy Meislin
[email protected]
SOURCE Lupus Research Alliance

细胞疗法免疫疗法临床研究临床结果AACR会议
2023-06-13
关注并星标CPHI制药在线 CAR-T细胞疗法已在复发性血液系统肿瘤的治疗中取得了显著的成功。不过,在使用CAR-T治疗的患者中,至少有50%的患者仍会出现复发或进展,主要原因在于CAR-T细胞的有限持久性、功能抑制和抗原逃逸。 有研究发现,在使用CD19 CAR-T治疗的急性淋巴细胞白血病(B-ALL)患者中,30%-95%的复发与细胞表面CD19缺失引起的疾病相关。 因此,研究者们开始探索双靶点CAR-T,即针对两种靶点特异性杀伤肿瘤细胞的CAR-T疗法。 在今年的ASCO会议上,亘喜生物以口头报告的形式在年会上公布了其CAR-T疗法GC012F治疗复发/难治性多发性骨髓瘤(R/R MM)多中心临床研究的长期随访数据。 GC012F是一款基于亘喜生物专有的FasTCAR技术平台开发的B细胞成熟抗原(BCMA)/CD19双靶点自体CAR-T细胞疗法,有望变革性地为癌症和自身免疫疾病治疗带来快速、深入且持久的效果,并具备差异化的安全性优势。 在这项单臂、开放标签、多中心的临床试验中,共入组29例R/R MM患者,中位随访时间为30.7个月,结果显示,患者的客观缓解率(ORR)为93.1%,其中89.6%的患者达到非常好的部分缓解(VGPR)及以上的疗效;82.8%的患者达到严格意义上的完全缓解(sCR)。 另在90%患者都属于高危的前提下, GC012F依然展现出了持久应答的疗效:中位缓解持续时间(mDOR)为37.0个月;中位无进展生存期(mPFS)为38.0个月;34%的患者维持微小残留病灶(MRD)-sCR状态超过12个月,预计这类患者在36个月时的PFS率可达100%。 安全性方面,GC012F在长期随访过程中未发现新的安全性事件。目前,GC012F正在开展多项研究,包括B细胞非霍奇金淋巴瘤(B-NHL)、系统性红斑狼疮(SLE)等。 目前,CD19是CAR-T开发中最为成熟的一个靶点,因此,基于CD19开发双靶点CAR-T细胞疗法是最为常见的开发路线。其中,最常见的靶点组合为CD19/CD22。 CD22在大多数B细胞恶性肿瘤细胞表面均有表达。对于CD19/CD22双靶点CAR-T细胞疗法来说,在CD19丢失的情况下,CD19/CD22 CAR-T还可以通过结合CD22来控制肿瘤的进展和复发。目前,国内布局CD19/CD22双靶点CAR-T的企业有优卡迪、驯鹿医疗、合源生物、北恒生物等。 优卡迪近日,优卡迪公布了串联其CD19/CD22 CAR-T细胞疗法治疗B-ALL的I/II期临床研究结果。研究共纳入219例患者,其中147例接受单纯CD19 CAR-T细胞治疗,51例接受串联CD19/CD22 CAR-T细胞治疗,21例接受序贯CD19/CD22 CAR-T细胞治疗。 结果显示,单纯CD19 CAR-T组、串联CD19/CD22 CAR-T组和序贯CD19/CD22 CAR-T组的CR分别为83.0%、98.0%和95.2%。串联CD19/CD22 CAR-T组临床疗效明显优于单纯CD19 CAR-T组,且与序贯CD19/CD22 CAR-T组疗效相似。高危因素患者CD19/CD22串联组的CR高于单纯CD19组(100.0% vs. 82.4%)。 单纯CD19 CAR-T组、串联CD19/CD22 CAR-T组和序贯CD19/CD22 CAR-T组的2年OS值分别为59.2%、76.3%和77.6%。在未接受同种异体HSCT移植(allo-HSCT)患者中,串联CD19/CD22 CAR-T组的中位OS显著优于单纯CD19 CAR-T组(未达到 vs 23.5个月)。 驯鹿医疗CT120是由驯鹿医疗研发的全人源CD19/CD22双靶点CAR-T产品。通过采用双靶点设计,能够减少现有 CAR-T疗法中因靶抗原丢失导致的肿瘤细胞逃逸问题,有望为患者带来更好的生存获益。通过采用全人源抗体序列,可以提高CAR-T的体内存续能力。 目前, CT120 已经在国内获批两项临床试验,分别用于 CD19/CD22阳性的复发/难治性B-NHL和复发/难治性B-ALL。在一项研究者发起的临床研究中,4例B-ALL患者在接受CT120治疗后,全部达到CR,未发生任何3级或3级以上的细胞因子释放综合征(CRS)不良反应。 合源生物HY004是合源生物研发的一款靶向CD19/CD22抗原的CAR-T,在体外利用慢病毒载体对患者自身T细胞进行基因修饰后而制备的细胞制剂,可以直接识别靶细胞表面的CD19和CD22分子,靶向杀伤效果更强,并通过减少肿瘤细胞的抗原逃逸而减少疾病复发和保持疗效持久。 在2022ASH年会上,合源生物公布了HY004在B细胞恶性肿瘤患者中的疗效数据。结果显示,6例R/R B-ALL患者接受了CAR-T细胞回输,ORR高达100%,6例患者均获得了MRD阴性的缓解,且3个月内未观察到严重CRS(≥3级)和任何级别的免疫效应细胞相关神经毒 性(ICANS)。 目前,HY004正在开展治疗成人R/R B-ALL和R/R NHL患者的治疗试验。 CAR-T细胞疗法已成为全球最热门的免疫疗法之一。尽管这些以单一抗原为靶点的CAR-T细胞疗法可以提供高应答率,但是接受这些CAR-T治疗的大部分患者也面临着肿瘤免疫逃逸的问题。抗原丢失或下调是单靶点CAR-T治疗后失败的主要机制。双靶点CAR-T则代表了一种可克服抗原调节并降低后续疾病复发风险的新策略。不过在双靶点CAR-T细胞治疗中,如何实现1+1>2,仍然需要对CAR靶点的选择以及CAR结构进行进一步的优化。 主要参考资料: 1、 Current Status and Perspectives of Dual-Targeting Chimeric Antigen Receptor T-Cell Therapy for the Treatment of Hematological Malignancies. Cancers (Basel).2022 Jul; 14(13): 3230. 2、 Sining Liu et al. (2023). Which one is better for refractory/relapsed acute B-cell lymphoblastic leukemia: Single-target (CD19) or dual-target (tandem or sequential CD19/CD22) CAR T-cell therapy? blood cancer journal.doi:https://doi-org.libproxy1.nus.edu.sg/10.1038/s41408-023-00819-5. 3、 Mackensen A, Müller F, Mougiakakos D, et al. Anti-CD19 CAR T cell therapy for refractory systemic lupus erythematosus. Nat Med 28, 2124-2132 (2022). https://doi-org.libproxy1.nus.edu.sg/10.1038/s41591-022-02017-5 . 【企业推荐】智药研习社近期课程报名来源:CPHI制药在线声明:本文仅代表作者观点,并不代表制药在线立场。本网站内容仅出于传递更多信息之目的。如需转载,请务必注明文章来源和作者。投稿邮箱:Kelly.Xiao@imsinoexpo.com▼更多制药资讯,请关注CPHI制药在线▼点击阅读原文,进入智药研习社~
细胞疗法ASCO会议临床结果免疫疗法临床1期
2022-11-07
CAR T-cell therapy clinical trial pipeline constitutes 193+ key companies continuously working towards developing 450+ CAR T-cell therapies, analyzes DelveInsight
LAS VEGAS, Nov. 7, 2022 /PRNewswire/ -- DelveInsight's
'
CAR T-cell Therapy Competitive Landscape – 2022
' report provides comprehensive global coverage of available, marketed, and pipeline CAR T-cell therapies in various stages of clinical development, major pharmaceutical companies are working to advance the pipeline space and future growth potential of the CAR T-cell therapy competitive domain.
Key Takeaways from the CAR T-cell Therapy Pipeline Report
Over
193+ CAR T companies are evaluating
450+ CAR T-cell therapies in various stages of development, and their anticipated acceptance in the CAR T-cell therapy market would significantly increase market revenue.
Leading CAR T companies such as
Alnylam Pharmaceuticals, JW Therapeutics, Gilead Sciences, Janssen Pharmaceuticals, Innovent Biologics, Sorrento Therapeutics, Cartesian Therapeutics, CASI Pharmaceuticals, Juventas Cell Therapy, Novartis, Poseida Therapeutics,Shanghai Unicar-Therapy Bio-medicine Technology, Sinobioway Cell Therapy Co., Ltd., Tessa Therapeutics, Wuhan Bio-Raid Biotechnology, Miltenyi Biomedicine, Bristol-Myers Squibb, Autolus Limited, Beijing Immunochina Medical Science and Technology, Carsgen Therapeutics, Cellular Biomedicine Group, Chongqing Precision Biotech, Eureka Therapeutics, Formula Pharmaceuticals, Guangzhou Bio-gene Technology, Hebei Senlang Biotechnology, Mustang Bio, MolMed, Aurora BioPharma, Atara Biotherapeutics, Autolus, Bellicum Pharmaceuticals, Kecellitics Biotech Company Ltd, Yake Biotechnology, Minerva Biotechnologies, Allogene Therapeutics, PersonGen BioTherapeutics (Suzhou), Precision BioSciences, Pregene (ShenZhen) Biotechnology Company, Shanghai GeneChem, Shanghai Longyao Biotechnology, Shenzhen BinDeBio, and others are evaluating novel CAR T-cell Therapy drugs candidate to improve the treatment landscape.
Key CAR T pipeline therapies in various stages of development include
Breyanzi, Kymriah, CT103A, CEA CAR-T, Descartes-11, CNCT19, CTL119, P-BCMA-101, CD19/CD20/CD22/CD30 CAR T-cell therapy, CD19-targeted CAR T-cells, EPCAM-targeted CAR-T cells, TT11, CD19+CD22 CAR-T cell sequential therapy, CART-19/22, MB-CART2019.1, JCAR017, AUTO4, AUTO3, IM19 CAR-T, CSG-CD19, CT053, Descartes-08, Orvacabtagene autoleucel, CAR-T CD30, PCAR-19B, BCMA CAR-T cells, CD123 CAR-T cells, CD19 CAR-T cells, ET140202, CIK-CAR.CD19, BG-T19, Autologous CD19-targeting CAR T cells (Senl-001), MB-102, Autologous CAR-T CD44v6 cell therapy, AU101, ATA2271, AU105, AUTO1, BPX-601, Anti-CD22 CAR, CAR-T cells targeting CD19 and CD22, huMNC2-CAR44 CAR T-cells, CD19-CART, ALLO-501A, AUTO1/22, ET 1402L1-CART, BPX-603, CAR-CD44v6, MB-106 (CD20 CAR), Anti-MUC1 CAR-T cells, PCAR-019, PBCAR0191, PBCAR20A, PBCAR269A, BCMA CAR T-cells, CAR19 CAR T cells, MG7-CART Cells, GPC3 – CART Cells, Anti-CD19 and Anti-CD20 CAR-T Cells, Humanized CD19 CAR-T cells, Dual Specificity CD19 and CD22 CAR-T Cell Immunotherapy, Mesothelin CAR-T cell therapy, and others.
In
May 2022, Novartis announced the US Food and Drug Administration (FDA) had granted accelerated approval for Kymriah (tisagenlecleucel) for the treatment of adult patients with relapsed or refractory (r/r) follicular lymphoma (FL) after two or more lines of systemic therapy. Kymriah is now FDA-approved in three indications and remains the only CAR-T cell therapy approved in both adult and pediatric settings.
In
April 2022, the FDA approved
axicabtagene ciloleucel (brand name Yescarta) for adult patients with large B-cell lymphoma that is refractory to first-line chemoimmunotherapy or relapses within 12 months of first-line chemoimmunotherapy. It is not indicated for treating patients with primary central nervous system lymphoma.
In
March 2022, JW Therapeutics announced that it had received the Investigational New Drug (IND) clearance from the National Medical Products Administration (NMPA) of China for a pivotal clinical trial of its anti-CD19 autologous chimeric antigen receptor T (CAR-T) cell immunotherapy product Carteyva (relmacabtagene autoleucel injection) in the treatment of second-line large B-Cell lymphoma.
In
February 2022, Fully human anti-B-cell maturation antigen (BCMA) chimeric antigen receptor (CAR) T-cell therapy (CT103A) received orphan drug designation (ODD) from the FDA for the treatment of relapsed and/or refractory multiple myeloma (R/R MM), according to a press release by IASO Biotherapeutics.
In
June 2021, based on
ZUMA-3 study data, the US FDA accepted the supplemental Biologics License Application (sBLA) and granted Priority Review designation for Tecartus for the treatment of adult patients with relapsed or refractory B-cell precursor ALL.
In
April 2021, the
Janssen Pharmaceutical Companies of
Johnson & Johnson announced that they had submitted a Marketing Authorisation Application (MAA) to the European Medicines Agency (EMA) seeking approval of cilta-cel for the treatment of patients with relapsed and refractory multiple myeloma.
In
March 2021, the FDA approved Abecma (idecabtagene vicleucel), a cell-based CAR T - Cell Therapy to treat adult patients with multiple myeloma who have not responded to or whose disease has returned after at least four prior lines (different types) of therapy. Abecma is the first cell-based CAR T - Cell Therapy approved by the FDA for treating multiple myeloma.
Request a sample and discover the recent advances in CAR T therapies @
CAR T-cell Therapy Competitive Landscape Report
CAR T-cell Therapy Overview
Chimeric antigen receptors (CARs) are recombinant antigen receptors that redirect the specificity and function of T lymphocytes and other immune cells in a single molecule. Cancer Immunotherapy is one of the most promising approaches for treating severe diseases (including cancer, autoimmune diseases, and allergic-hypersensitivity reactions) because it uses and improves the immune system's standard capacity. CAR T-cells are proteins that are fusions of a specific monoclonal antibody's single-chain fragment variable and one or more T-cell receptor intracellular signaling domains. A CAR combines antigen-binding domains—most commonly, a single-chain variable fragment (scFv) derived from antibody variable domains—with TCR chain signaling domains and costimulatory domains from receptors such as CD28, OX40, and CD137.
For more information about CAR T-cell therapy drugs; visit @
CAR T-cell Therapy Process
CAR T-cell Therapy Pipeline Analysis: Drug Profile
JWCAR029: JW Therapeutics
JW Therapeutics drug JWCAR029 is a CAR-T cell product that targets CD19 and is intended to treat advanced lymphoma and leukemia (Second-line therapy or greater). The molecule is currently in phase II of development. JWCAR029 is initially being investigated for the treatment of B-cell malignancies, with a focus on relapsed and refractory DLBCL. The National Medical Products Administration ("NMPA") accepted for review its NDA for relma-cel as a third-line treatment for DLBCL in June 2020.
KTE-X19: Gilead Sciences
Gilead Sciences drug KTE-X19 is an autologous CD19 CAR T-cell therapy under investigation. The drug is manufactured using the XLP process, including T-cell selection and lymphocyte enrichment. Lymphocyte enrichment is required in certain B-cell malignancies for which KTE-X19 is being studied. KTE-X19 is currently in Phase II clinical trials for the treatment of both adult and pediatric acute lymphocytic leukemia. Brexucabtagene autoleucel (formerly KTE-X19; Tecartus) has been approved by the FDA for the treatment of adult patients with relapsed or refractory mantle cell lymphoma (MCL).
A snapshot of the CAR T-cell Therapy Pipeline Drugs mentioned in the report:
Learn more about FDA approved CAR T-cell therapy @
CAR T Clinical Trials
Scope of the CAR T-cell Therapy Competitive Landscape Report
Coverage: Global
Key CAR T-cell Therapy Companies: Alnylam Pharmaceuticals, JW Therapeutics, Gilead Sciences, Janssen Pharmaceuticals, Innovent Biologics, Sorrento Therapeutics, Cartesian Therapeutics, CASI Pharmaceuticals, Juventas Cell Therapy, Novartis, Poseida Therapeutics,Shanghai Unicar-Therapy Bio-medicine Technology, Sinobioway Cell Therapy Co., Ltd., Tessa Therapeutics, Wuhan Bio-Raid Biotechnology, Miltenyi Biomedicine, Bristol-Myers Squibb, Autolus Limited, Beijing Immunochina Medical Science and Technology, Carsgen Therapeutics, Cellular Biomedicine Group, Chongqing Precision Biotech, Eureka Therapeutics, Formula Pharmaceuticals, Guangzhou Bio-gene Technology, Hebei Senlang Biotechnology, Mustang Bio, MolMed, Aurora BioPharma, Atara Biotherapeutics, Autolus, Bellicum Pharmaceuticals, Kecellitics Biotech Company Ltd, Yake Biotechnology, Minerva Biotechnologies, Allogene Therapeutics, PersonGen BioTherapeutics (Suzhou), Precision BioSciences, Pregene (ShenZhen) Biotechnology Company, Shanghai GeneChem, Shanghai Longyao Biotechnology, Shenzhen BinDeBio, and others
Key CAR T-cell Therapies in Pipeline: Breyanzi, Kymriah, CT103A, CEA CAR-T, Descartes-11, CNCT19, CTL119, P-BCMA-101, CD19/CD20/CD22/CD30 CAR T-cell therapy, CD19-targeted CAR T-cells, EPCAM-targeted CAR-T cells, TT11, CD19+CD22 CAR-T cell sequential therapy, CART-19/22, MB-CART2019.1, JCAR017, AUTO4, AUTO3, IM19 CAR-T, CSG-CD19, CT053, Descartes-08, Orvacabtagene autoleucel, CAR-T CD30, PCAR-19B, BCMA CAR-T cells, CD123 CAR-T cells, CD19 CAR-T cells, ET140202, CIK-CAR.CD19, BG-T19, Autologous CD19-targeting CAR T cells (Senl-001), MB-102, Autologous CAR-T CD44v6 cell therapy, AU101, ATA2271, AU105, AUTO1, BPX-601, Anti-CD22 CAR, CAR-T cells targeting CD19 and CD22, huMNC2-CAR44 CAR T-cells, CD19-CART, ALLO-501A, AUTO1/22, ET 1402L1-CART, BPX-603, CAR-CD44v6, MB-106 (CD20 CAR), Anti-MUC1 CAR-T cells, PCAR-019, PBCAR0191, PBCAR20A, PBCAR269A, BCMA CAR T-cells, CAR19 CAR T cells, MG7-CART Cells, GPC3 – CART Cells, Anti-CD19 and Anti-CD20 CAR-T Cells, Humanized CD19 CAR-T cells, Dual Specificity CD19 and CD22 CAR-T Cell Immunotherapy, Mesothelin CAR-T cell therapy, and others.
Dive deep into rich insights for CAR T-cell therapy drugs; visit @
FDA-approved CAR T-cell Therapy
Table of Contents
For further information on the CAR T-cell therapy pipeline therapeutics, reach out @
CAR T-cell Therapy Clinical Trials
Related Reports
CAR T-cell Therapy for Acute Lymphoblastic Leukemia Market
CAR T-cell Therapy for Acute Lymphoblastic Leukemia Market Insights, Epidemiology, and Market Forecast – 2032 report deliver an in-depth understanding of the disease, historical and forecasted epidemiology, as well as the market trends, market drivers, market barriers, and key CAR T-cell therapy for acute lymphoblastic leukemia companies, including
Autolus, Pepromene Bio, Actinium Pharmaceuticals, among others.
CAR T-cell Therapy for Multiple Myeloma Market
CAR T-cell Therapy for Multiple Myeloma Market Insights, Epidemiology, and Market Forecast – 2032 report delivers an in-depth understanding of the disease, historical and forecasted epidemiology, as well as the market trends, market drivers, market barriers, and key CAR T-cell therapy for multiple myeloma companies, including
Novartis, Yake Biotech, Celgene Corporation, among others.
CAR T-cell Therapy for Non-Hodgkin's Lymphoma Market
CAR T-cell Therapy for Non-Hodgkin's Lymphoma Market Insights, Epidemiology, and Market Forecast – 2032 report delivers an in-depth understanding of the disease, historical and forecasted epidemiology, as well as the market trends, market drivers, market barriers, and key CAR T-cell therapy for non-Hodgkin's lymphoma companies, including
Juno Therapeutics, Allogene Therapeutics, Caribou Biosciences, among others.
CAR T-cell Therapy for Acute Lymphoblastic Leukemia Pipeline
CAR T-cell Therapy for Acute Lymphoblastic Leukemia Pipeline Insight – 2022 report provides comprehensive insights about the pipeline landscape, pipeline drug profiles, including clinical and non-clinical stage products, and the key CAR T-cell therapy for acute lymphoblastic leukemia companies, including
Autolus, Pepromene Bio, Actinium Pharmaceuticals, among others.
CAR T-cell Therapy for Multiple Myeloma Pipeline
CAR T-cell Therapy for Multiple Myeloma Pipeline Insight – 2022 report provides comprehensive insights about the pipeline landscape, pipeline drug profiles, including clinical and non-clinical stage products, and the key CAR T-cell therapy for multiple myeloma companies, including
Novartis, Yake Biotech, Celgene Corporation, among others.
CAR T-cell Therapy for Non-Hodgkin's Lymphoma Pipeline
CAR T-cell Therapy for Non-Hodgkin's Lymphoma Pipeline Insight – 2022 report provides comprehensive insights about the pipeline landscape, pipeline drug profiles, including clinical and non-clinical stage products, and the key CAR T-cell therapy for non-Hodgkin's lymphoma companies, including
Juno Therapeutics, Allogene Therapeutics, Caribou Biosciences, among others.
Other Trending Reports
Goitre Market
|
Thymus Cancer Market
|
US Healthcare Outlook Report
|
Venous Stenosis Market
|
Negative Pressure Wound Therapy Systems Market
|
Global Kinase Inhibitor in Autoimmune Diseases Market
|
Metrorrhagia Market
|
Dysfunctional Uterine Bleeding Market
|
Hypereosinophilic Syndrome Market
|
Age-related Vision Dysfunction Market
|
Dental Lasers Market
|
CRISPR Therapies Pipeline Insight
|
Cell And Gene Therapy For Multiple Myeloma Market
|
Drug Hypersensitivity Market
|
Dysthymia Market
|
Persistent Depressive Disorder Market
|
Cancer Vaccines Market
|
Weight Loss/Weight Management (Obesity) Market
|
Food Allergy Market
|
Obsessive-Compulsive Disorder Market
|
Tumor Ablation Market
|
Physiotherapy Equipment Market
|
Chimeric Antigen Receptor (CAR) T-Cell Therapy Market
|
Anti-hypertension Market
|
Radiofrequency Ablation Devices Market
|
Global Messenger RNA (mRNA)-based Vaccines and Therapeutics Market
|
Gastro Intestinal Bleeding Market
|
Trastuzumab Biosimilars Insight
|
Varicose Veins Market
|
Germ Cell Tumor Market
|
Intracardiac Echocardiography Devices Market
|
India Healthcare Report
|
Crows Feet Market
|
Seborrhoeic Dermatitis Market
|
Injectable Drug Delivery Devices Market
|
Structural Heart Devices Market
|
Substance (Drug) Abuse Market
|
Insulin Glargine Biosimilar Insight
About DelveInsight
DelveInsight is a leading Business Consultant, and Market Research firm focused exclusively on life sciences.
Connect with us at LinkedIn
Contact Us
Shruti Thakur
[email protected]
+1(919)321-6187
Logo:
SOURCE DelveInsight Business Research, LLP
基因疗法抗体孤儿药生物类似药细胞疗法
100 项与 Anti-CD19 CAR T-cell therapy (Institute of Hematology and Blood Diseases Hospital of the Chinese Academy of Medical Sciences ) 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 成人急性淋巴细胞白血病 | 临床2期 | 中国 | 2024-06-25 | |
| 成人急性淋巴细胞白血病 | 临床2期 | 中国 | 2024-06-25 | |
| 前体B细胞急性淋巴细胞白血病 | 临床2期 | 中国 | 2024-06-25 | |
| 前体B细胞急性淋巴细胞白血病 | 临床2期 | 中国 | 2024-06-25 | |
| 难治性B细胞淋巴瘤 | 临床2期 | 中国 | 2024-04-30 | |
| 特发性炎症性肌病 | 临床1期 | - | - | 2024-11-15 |
| 显微镜下多血管炎 | 临床1期 | - | - | 2024-11-15 |
| 系统性硬皮病 | 临床1期 | - | - | 2024-11-15 |
| 干燥综合征 | 临床1期 | - | - | 2024-11-15 |
| 系统性红斑狼疮 | 临床1期 | - | - | 2024-11-15 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
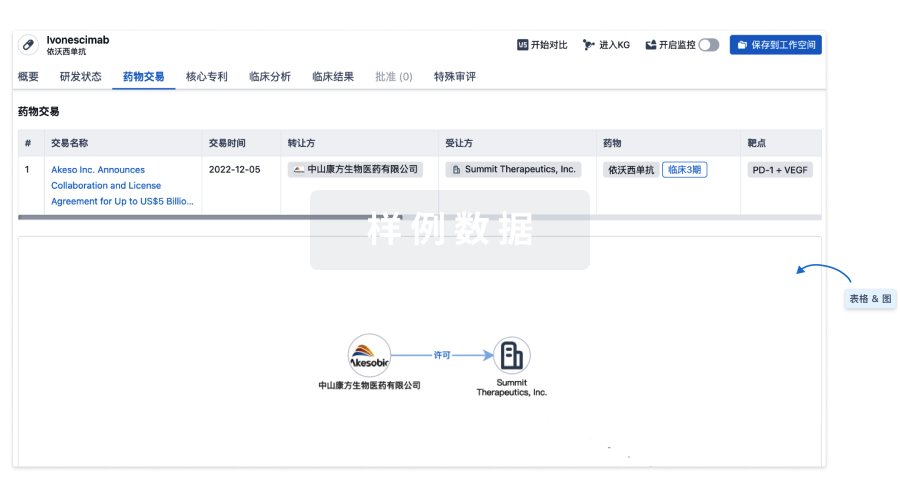
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
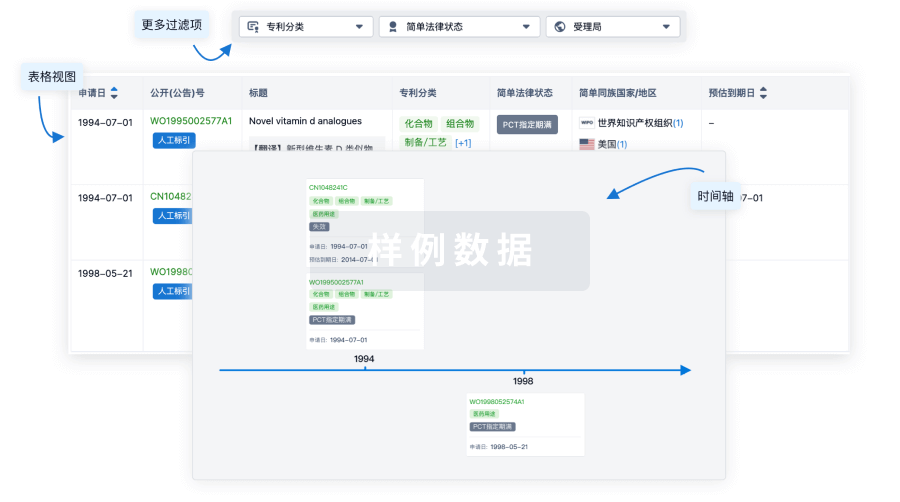
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用