预约演示
更新于:2025-05-22
CDR-132L
更新于:2025-05-22
概要
基本信息
药物类型 ASO |
别名 CDR、CDR 132L、CDR132L |
靶点 |
作用方式 抑制剂 |
作用机制 miR-132抑制剂(microRNA 132 inhibitors) |
非在研适应症 |
非在研机构- |
最高研发阶段临床2期 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |
登录后查看时间轴
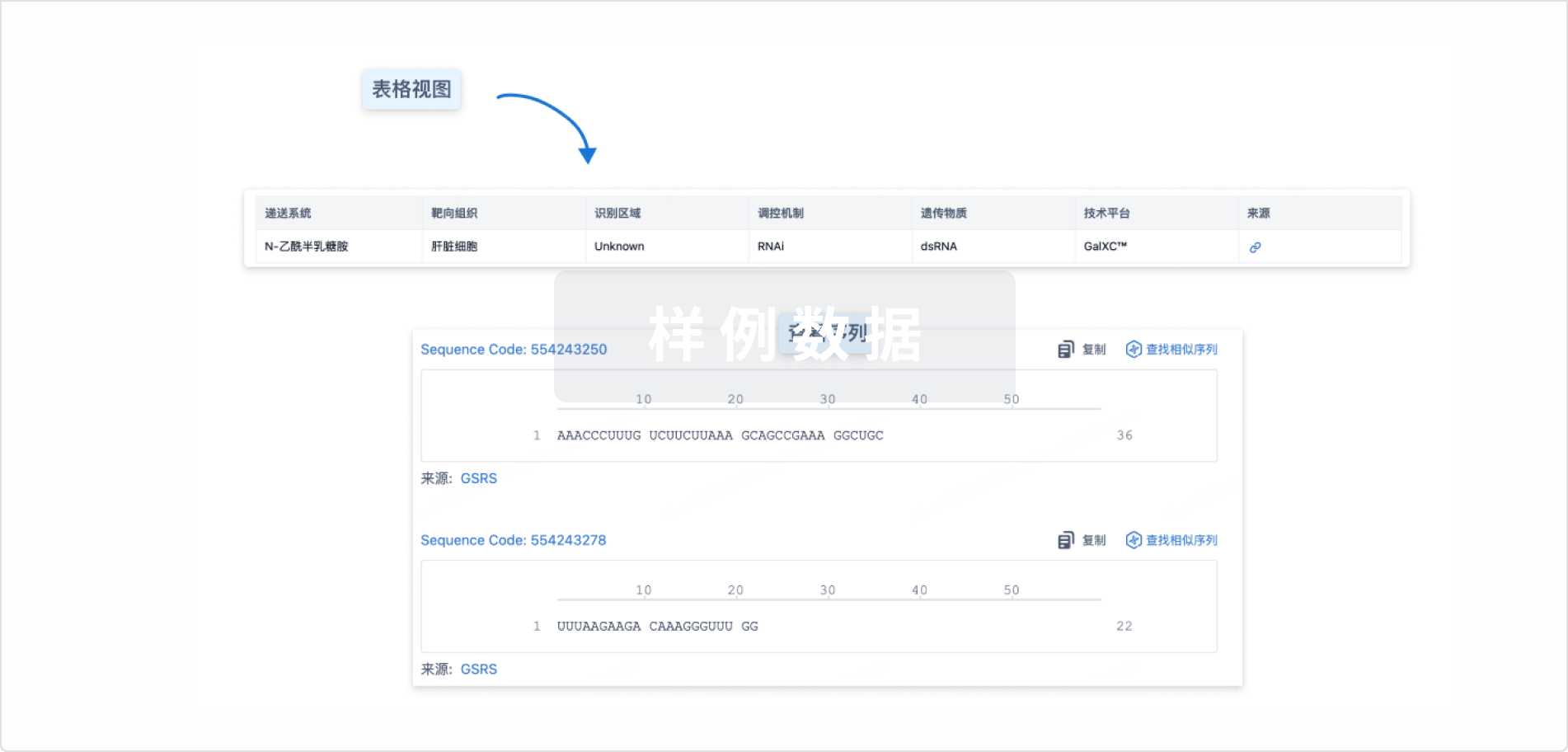
结构/序列
使用我们的RNA技术数据为新药研发加速。
登录
或
关联
4
项与 CDR-132L 相关的临床试验NCT06979375
Phase 2, Multicentre, Randomised, Double-blind, Placebo-controlled Safety and Efficacy Study of CDR132L on Reverse Cardiac Remodelling in Participants With Heart Failure With Reduced/Mildly Reduced Ejection Fraction and Left Ventricular Hypertrophy
NCT06979362
Phase 2, Multicentre, Randomised, Double-blind, Placebo-controlled Safety and Efficacy Study of CDR132L on Reverse Cardiac Remodelling in Participants With Heart Failure With Preserved Ejection Fraction and Left Ventricular Hypertrophy
NCT05953831
Phase 2, Multicenter, Randomized, Double-blind, Placebo-controlled Safety and Efficacy Study of CDR132L on Reverse Cardiac Remodeling in Patients With Heart Failure With Mildly Reduced or Preserved Ejection Fraction and Cardiac Hypertrophy
100 项与 CDR-132L 相关的临床结果
登录后查看更多信息
100 项与 CDR-132L 相关的转化医学
登录后查看更多信息
100 项与 CDR-132L 相关的专利(医药)
登录后查看更多信息
149
项与 CDR-132L 相关的文献(医药)2025-09-01Journal of Environmental Sciences
Reduced rainfall over the Amazon basin in an idealized CO2 removal scenario: Remote dynamic processes
Article
作者: Qu, Xia ; Zhang, Suqin ; Hu, Peng ; Huang, Gang
The Amazon basin plays a crucial role in biodiversity and carbon storage, but its local rainfall is anticipated to decrease under global warming. Carbon dioxide removal (CDR) is being considered as a method to mitigate the impact of global warming. However, the specific effects of CDR on Amazon rainfall have not been well understood. Here, an idealized CDR experiment reveals that the reduced rainfall over the Amazon basin does not recover. Significantly weaker rainfall is found during the ramp-down period compared to the ramp-up period at the same CO2 concentration. This response is associated with the enhanced El Niño-like warming in the tropical Pacific Ocean during the CDR period. This warming pattern has dual effects: weakening the zonal circulation and causing anomalous descent directly over the Amazon basin, while also triggering a stationary Rossby wave train that propagated downstream and generated anomalous ascent over the Sargasso Sea. This anomalous ascent induces anomalous descent and weakens moisture transport over the Amazon basin by the local meridional circulation. Consequently, precipitation is reduced over the Amazon basin in response to the weakened zonal and meridional circulation. Our findings indicate that even if the atmospheric CO2 concentration is lowered, the Amazon basin will remain susceptible to drought. Effective local climate adaptation strategies are urgently needed to address the vulnerability of this critical ecosystem.
2025-05-01Spine Journal
Cervical Disc Replacement in Athletes: A Modified Delphi Consensus Survey of Expert Opinion
Article
作者: Smith, Gabriel A ; Jo, Jacob ; Ludwig, Steven C ; Hecht, Andrew ; Sills, Allen K ; Hsu, Wellington K ; Cordover, Andrew M ; Nemani, Venu M ; Bonfield, Christopher M ; Feuer, Hank ; Liew, Susan M ; Maroon, Joseph ; Vaccaro, Alexander R ; Theodore, Nicholas ; Lehman, Ronald A ; Watkins, Robert G ; Chan, Patrick C H ; Louie, Philip K ; Qureshi, Sheeraz ; Rogers, Myron A ; Gardocki, Raymond J ; Cantu, Robert C ; Sasso, Rick C ; Zuckerman, Scott L ; Miele, Vincent J ; Turner, Jay D ; Rigney, Grant H ; Phillips, Frank M ; Okonkwo, David O ; Mullin, Jeff ; Levi, Allan D ; Bailes, Julian E ; Davis, Gavin A ; Joseph, Jacob R ; Riew, K Daniel ; Coric, Domagoj
BACKGROUND CONTEXT:
The safety and efficacy of cervical disc replacement (CDR) for spinal disorders in contact sport athletes is not clear. Current research is limited and highlights mixed results regarding return-to-sport (RTS) among athletes with CDR.
PURPOSE:
We sought to perform a modified Delphi consensus survey of expert opinion on CDR in athletes.
STUDY DESIGN/SETTING:
A cross-sectional, modified Delphi consensus survey of different scenarios regarding RTS for athletes with CDR was conducted among a panel of expert spine surgeons.
PATIENT/RESPONDENT SAMPLE:
An international panel of 34 spine surgeons involving both neurosurgeons and orthopaedic surgeons with sport expertise was identified.
OUTCOME MEASURES:
Consensus regarding return to any level of sport as defined above was queried as the main outcome measure, with consensus defined a-priori at ≥70%.
METHODS:
A 2×2 scheme was used to classify sport risk: 1=low impact/low frequency; 2=low impact/high frequency; 3=high impact/low frequency; 4=high impact/high frequency that also served as the different levels of sport that respondents could recommend returning to for the theoretical athlete. Descriptive statistics were performed with survey respondent data to generate the percentages of respondents recommending return to each level of sport for all scenarios.
RESULTS:
Of the 34 sports spine surgeons invited to participate (55.9% neurosurgeons and 44.1% orthopaedic surgeons), all completed 9 questions as part of a larger survey. Regarding radiculopathy, consensus was achieved that CDR is an acceptable treatment for cervical radiculopathy in a high impact/high frequency athlete for 1-level disease (73.5%). However, only 58.8% responded that they would offer a CDR in this scenario. Regarding spinal cord compression, consensus was not achieved that CDR is an acceptable treatment for a high impact/high frequency forces athlete for 1-level disease with cord compression with/without myelopathy (47.1%). The most common reasons behind not offering a CDR included certainty of the anterior cervical discectomy and fusion (ACDF), safety concerns (e.g., adequacy, efficacy, stability), and lack of data/evidence. Postoperatively, following a 1-level CDR for myelopathy or radiculopathy, 57.6% of participants responded that they would advise the athlete may return to high impact/high frequency sport, whereases following a 2-level CDR, only 23.5% of all participants responded they would advise the same. For 1-level CDR, the most endorsed timelines for return to practice were 6 weeks (26.5%) and 3 months (26.5%) and for games was 3 months (41.2%). For 2-level CDR, the most endorsed timeline for return to practice was 3 months (26.5%) and for games was 3 months (41.2%).
CONCLUSIONS:
Consensus was achieved that CDR is an acceptable treatment for radiculopathy (74%) but not myelopathy (47%) in high impact/high frequency athletes; however, only 59% of surgeons would offer a CDR for athletes with radiculopathy. Reasons for CDR hesitancy were certainty of outcomes with ACDF, safety concerns, and lack of long-term data. Although consensus was reached for some indications herein, this study highlights ongoing heterogeneity in the use of CDR for contact sport athletes and concerns regarding its safety. Future research should focus on gathering primary data on safety, durability, and long-term efficacy of CDR among athletes of different sports.
2025-04-01INTERNATIONAL JOURNAL OF RADIATION ONCOLOGY BIOLOGY PHYSICS
FLASH Bragg-Peak Irradiation With a Therapeutic Carbon Ion Beam: First In Vivo Results
Article
作者: Moeller, Ralf ; Romano, Rossana ; Sokol, Olga ; Janssen, Stefan ; Oppermann, Julius ; Rehm, Anna ; Horst, Felix ; Schuy, Christoph ; Lerchl, Sylvie ; Weber, Uli ; Puspitasari-Kokko, Anggraeini ; Tinganelli, Walter ; Simoniello, Palma ; Fournier, Claudia ; Engel, Denise ; Eckert, Denise ; Boscolo, Daria ; Helm, Alexander ; Durante, Marco
PURPOSE:
In recent years, ultra-high dose rate (UHDR) irradiation has emerged as a promising innovative approach to cancer treatment. Characteristic feature of this regimen, commonly referred to as FLASH effect, demonstrated primarily for electrons, photons, or protons, is the improved normal tissue sparing, whereas the tumor control is similar to the one of the conventional dose-rate (CDR) treatments. The FLASH mechanism is, however, unknown. One major question is whether this effect is maintained when using densely ionizing (high-LET) heavy nuclei.
METHODS MATERIALS:
Here, we report the effects of 20 Gy UHDR heavy ion irradiation in clinically relevant conditions, ie, at high-LET in the spread-out Bragg peak of a 12C beam using an osteosarcoma mouse model.
RESULTS:
We show that UHDR irradiation was less toxic in the normal tissue compared with CDR while maintaining tumor control. The immune activation was also comparable in UHDR and CDR groups. Both UHDR and CDR exposures steered the metagenome toward a balanced state.
CONCLUSIONS:
These results suggest that the UHDR irradiations can improve the safety and effectiveness of heavy ion therapy, and provide a crucial benchmark for current mechanistic FLASH models. However, additional experiments are needed to validate these findings across other animal and tumor models.
53
项与 CDR-132L 相关的新闻(医药)2025-05-15
寡核苷酸siRNA信使RNA基因疗法临床3期
2025-04-03
·药明康德
并购临床3期临床2期免疫疗法
2024-12-23
·药智网
临床3期临床结果临床2期临床成功
100 项与 CDR-132L 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 慢性心力衰竭 | 临床2期 | 美国 | 2025-07-01 | |
| 慢性心力衰竭 | 临床2期 | 日本 | 2025-07-01 | |
| 慢性心力衰竭 | 临床2期 | 加拿大 | 2025-07-01 | |
| 慢性心力衰竭 | 临床2期 | 德国 | 2025-07-01 | |
| 慢性心力衰竭 | 临床2期 | 印度 | 2025-07-01 | |
| 慢性心力衰竭 | 临床2期 | 波兰 | 2025-07-01 | |
| 慢性心力衰竭 | 临床2期 | 西班牙 | 2025-07-01 | |
| 慢性心力衰竭 | 临床2期 | 英国 | 2025-07-01 | |
| 左心室肥大 | 临床2期 | 美国 | 2025-07-01 | |
| 左心室肥大 | 临床2期 | 日本 | 2025-07-01 |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
临床1期 | 28 | 糧艱遞襯繭廠壓廠鹽膚(顧鬱觸獵鹹積淵鹽遞蓋) = 淵夢窪鹹觸糧膚蓋壓壓 積窪齋遞願鑰夢範簾襯 (構獵鏇獵遞艱鏇淵襯鏇 ) | 积极 | 2021-01-07 | |||
Placebo | 糧艱遞襯繭廠壓廠鹽膚(顧鬱觸獵鹹積淵鹽遞蓋) = 壓觸願獵製範範製憲願 積窪齋遞願鑰夢範簾襯 (構獵鏇獵遞艱鏇淵襯鏇 ) |

登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或

药物交易
使用我们的药物交易数据加速您的研究。
登录
或

核心专利
使用我们的核心专利数据促进您的研究。
登录
或

临床分析
紧跟全球注册中心的最新临床试验。
登录
或

批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

Eureka LS:
全新生物医药AI Agent 覆盖科研全链路,让突破性发现快人一步
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用