预约演示
更新于:2025-03-29
TC-100
更新于:2025-03-29
概要
基本信息
原研机构 |
在研机构 |
非在研机构- |
最高研发阶段临床前 |
首次获批日期- |
最高研发阶段(中国)- |
特殊审评- |

关联
100 项与 TC-100 相关的临床结果
登录后查看更多信息
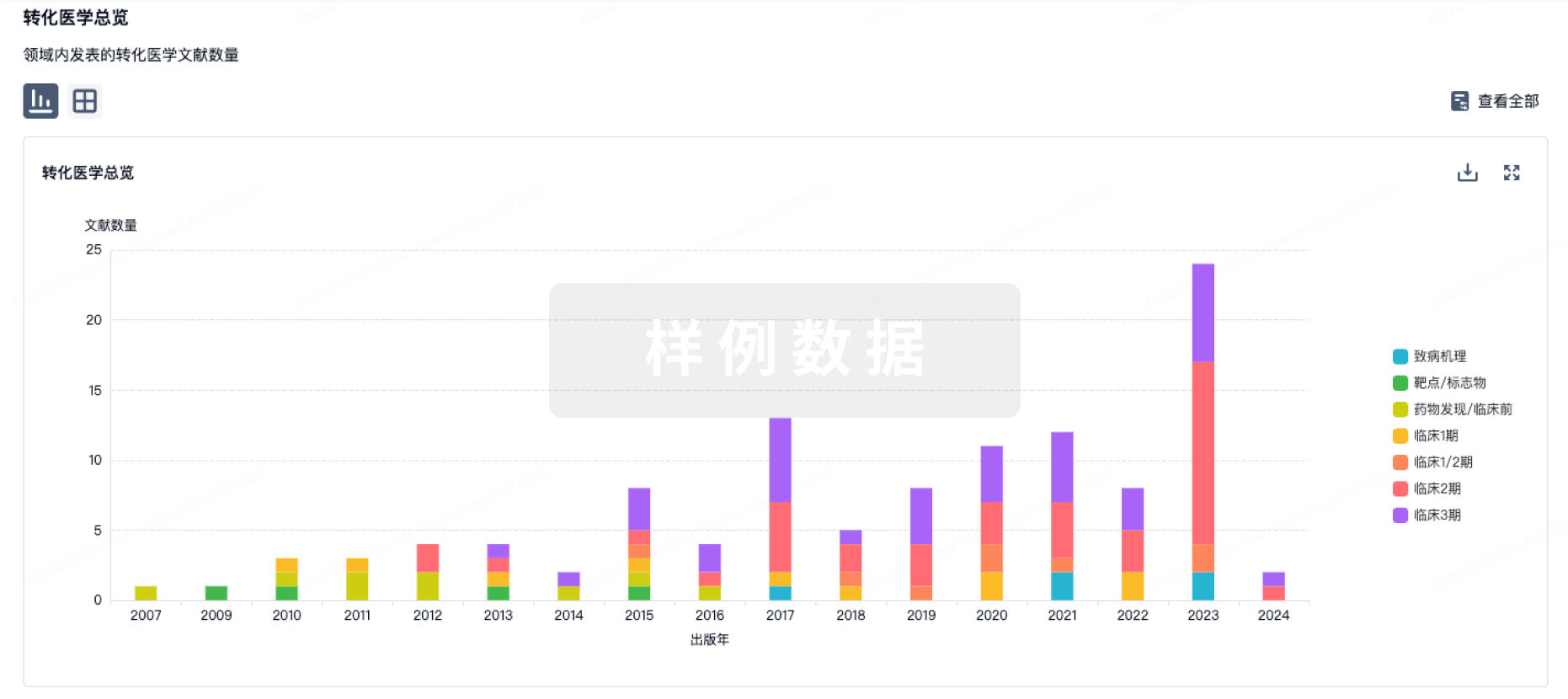
100 项与 TC-100 相关的转化医学
登录后查看更多信息
100 项与 TC-100 相关的专利(医药)
登录后查看更多信息
59
项与 TC-100 相关的文献(医药)2024-10-19·Hospital practice (1995)
An insight into the updated pharmacotherapy of metabolic-associated fatty liver disease (MAFLD) or metabolic dysfunction-associated steatohepatitis (MASH) in lean individuals: a review
Review
作者: Bandyopadhyay, Sanjay ; Das, Saibal ; Samajdar, Shambo Samrat ; Chaudhuri, Sirshendu
Metabolic-associated fatty liver disease (MAFLD) or metabolic dysfunction-associated steatohepatitis (MASH) in lean individuals represents a distinctive subset of MASH. Current pharmacotherapies, for MASH as demonstrated in clinical trials, predominantly target obese patients with limited consideration for lean MASH. We aimed to systematically review the literature on the pharmacotherapy of lean MASH. We searched standard medical databases, such as PubMed, Embase, Scopus, Cochrane CENTRAL, and ClinicalTrials.gov to identify eligible studies published in English up to 31 December 2023 regarding the effect of pharmacological interventions in individuals with lean MASH. We have summarized the role of various drug classes including peroxisome proliferator-activated receptor agonists, glucagon-like peptide-1 receptor agonists, sodium-glucose cotransporter 2 inhibitors, vitamin E, farnesoid X receptor agonists, selective thyroid hormone receptor-β agonists, and selective cholesterol absorption inhibitors. Consequently, lifestyle interventions, encompassing dietary modifications, exercise, and weight loss particularly directed at visceral obesity or achieving a reduction in body weight are recommended for all non-obese individuals with MASH. A highlight on the only available treatment recommendation for lean MASH is also presented. The available evidence regarding the efficacy of various drugs for the treatment of lean MASH is limited. Conclusive evidence is warranted from clinical trials exclusively involving lean individuals with MASH.
2024-06-28·Journal of Clinical and Translational Hepatology
Progress in the Management of Patients with Cholestatic Liver Disease: Where Are We and Where Are We Going?
Review
作者: Luo, Xin ; Lu, Lun-Gen
Cholestatic liver disease is a group of diseases in which bile acid accumulates in the liver for various reasons, resulting in abnormal liver biochemical indicators and histological damage. Cholestasis can be divided into intrahepatic cholestasis and extrahepatic cholestasis, which will contribute to liver damage and progress to liver fibrosis and cirrhosis. Primary biliary cholangitis (PBC) and primary sclerosing cholangitis are the two most typical cholestatic liver diseases. Ursodeoxycholic acid is currently the first-line treatment for PBC, while obeticholic acid, budesonide and fibrates have also shown good potential in the treatment of PBC. There are currently no official drugs approved to treat primary sclerosing cholangitis, and the use of ursodeoxycholic acid may have certain clinical benefits. At present, progress has been made in new treatment directions for cholestatic liver disease, including fibroblast growth factor 19, cholestyramine, S-adenosyl-L-methionine, steroid drugs, farnesoid X receptor agonists, and more. Considerable progress has been made in the management of cholestatic liver disease but there are still many opportunities and challenges. In this review, we summarized the recommended guidelines for the management of cholestatic disease and the progress of new drug research and development, in order to provide an important reference for the clinical practice of cholestatic liver disease.
2024-06-02·Expert opinion on investigational drugs
Investigational farnesoid X receptor agonists for the treatment of primary biliary cholangitis
Review
作者: Gochanour, Eric M ; Akepati, Prithvi Reddy
INTRODUCTION:
Up to 40% of Primary biliary cholangitis (PBC) patients have a suboptimal response to Ursodeoxycholic acid (UDCA). Close to half of such patients show a remarkable improvement when additionally treated with Obeticholic acid (OCA) but have a dose-dependent increase of pruritus. This relative success of OCA, a first-in-class Farnesoid receptor (FXR) agonist, has positioned FXR as an attractive target for drug development. Novel candidates have since emerged, providing hope for this subgroup of patients who lack effective and safe treatments.
AREAS COVERED:
We discussed the role of bile acids in PBC pathogenesis and how the FXR agonists provide therapeutic value by affecting bile acid synthesis and transport. Novel FXR agonists undergoing pre-clinical and clinical trials for PBC were enlisted via literature search by including the terms 'FXR agonists,' 'FXR PBC,' 'PBC clinical trials' on PubMed, MEDLINE via Ovid, and Clinicaltrials.gov.
EXPERT OPINION:
Novel FXR agonists currently under investigation for PBC improve the disease surrogate markers in early trials. However, as with OCA, pruritus remains a concern with the newer drugs despite targeted chemical modifications to increase FXR specificity. Directing future resources toward studying the molecular mechanisms behind pruritus may lead to better drug design and efficacious yet safer drugs.
2
项与 TC-100 相关的新闻(医药)2022-11-08
INT-787 is a selective next generation FXR agonist invented by TES Pharma and licensed to Intercept Pharmaceuticals
INT-787 has shown strong anti-fibrotic and anti-inflammatory effects in animal models
TES Pharma is dedicated to the identification of novel therapeutic targets and the discovery and development of new molecules to efficiently address the needs of patients with serious oncological and metabolic conditions
PERUGIA, Italy, Nov. 8, 2022 /PRNewswire/ -- TES Pharma Srl, an Italian biotechnology company focused on the discovery and development of novel drug products for the treatment of diseases of high unmet medical need, congratulates Intercept Pharmaceuticals, Inc., on the presentation of data from their ongoing first-in-human study of INT-787 and the initiation of the phase 2a FRESH (FxR Effect on Severe Alcohol-Associated Hepatitis) study, a trial evaluating the safety, tolerability, efficacy and pharmacokinetics of INT-787 in subjects with sAH. INT-787 is a selective next generation Farnesoid X Receptor (FXR) agonist invented by TES Pharma, and licensed to Intercept Pharmaceuticals within the framework of a licence and collaboration agreement. Details of the clinical studies can be found at .
Professor Roberto Pellicciari, the founder and CEO of TES Pharma, is also the inventor of obeticholic acid (OCA), a prototypic bile acid derived FXR agonist which is approved for the treatment of primary biliary cholangitis (PBC) and commercialised by Intercept Pharmaceuticals in the United States. PBC is a progressive autoimmune disease that damages the bile ducts in the liver and is a leading cause of chronic liver disease leading to liver transplantation.
INT-787 has distinct pharmacological properties that differ from those of OCA and has shown strong anti-fibrotic and anti-inflammatory effects in animal models. Data from a murine NASH model comparing OCA and INT-787 were also presented at the American Association for the Study of Liver Diseases (AASLD) meeting.
"We are proud of the work we do at TES Pharma, and very pleased about the ongoing first-in-human study of INT-787 and the initiation of the Phase 2a FRESH study in patients with severe alcohol-associated hepatitis, important milestones that encourage us to continue our mission to find new treatments to improve people's lives, especially for patients suffering from serious diseases", said Prof. Pellicciari.
TES Pharma is a research-based biotech company, located in Perugia (Italy), dedicated to the identification of novel therapeutic targets and the discovery and development of new molecules to efficiently address the needs of patients with serious oncological and metabolic conditions. More information about TES Pharma can be found at .
TES Pharma was founded in 2011 by Prof. Pellicciari together with Drs. Antimo Gioiello, Antonio Macchiarulo, and Janet Robertson. Prior to founding TES Pharma, Prof. Pellicciari led the Medicinal Chemistry Research Group at the Department of Chemistry and Drug Technologies of the University of Perugia.
CONTACT:
Prof. Roberto Pellicciari
rpellicciari@tespharma.com ,
Phone: +39 075 6978111
E: info@tespharma.com
F: +39 075 6978882
GSM: +39 366 9057122
Logo -
View original content to download multimedia:
SOURCE TES Pharma
合作
2021-10-04
Shares of Enanta Pharmaceuticals are falling this morning after the company announced plans to scrap the development of its two clinical stage farnesoid X receptor (FXR) agonists being developed as a potential treatment for non-alcoholic steatohepatitis (NASH).
Instead of continuing to develop the two different assets, EDP-305 and EDP-297, the company intends to seek an out-licensing deal that will further advance the research it began. Enanta plans to maintain its focus and resources on therapies aimed at hepatitis B virus and infectious respiratory diseases, including respiratory syncytial virus (RSV) and SARS-CoV-2, the virus that causes COVID-19.
This morning, the Watertown, Mass.-based company said it came to its decision following a preplanned examination from a Phase IIb study of EDP-305, a monotherapy FXR agonist treatment. Although its clinical data determined that a 1 mg dose of the experimental drug provided the best safety and efficacy results, the company decided to scrap the development of the program. And that likely means that the data was not strong enough for Enanta to continue to develop the asset on its own.
Jay R. Luly, president and chief executive officer of Enanta Pharmaceuticals, believes that the company's FXR agonists will likely do well as part of a combination treatment for NASH, a growing health concern that currently affects about 16 million people in the United States.
EDP-305 was being developed as a monotherapy and EDP-297 was being developed as a follow-on treatment. Luly said both of the FXR agonists are “well-positioned to be an important component of a combination therapy to bring a much-needed treatment to patients with NASH.”
The treatment, however, will have to be developed by another company. Luly pointed to the complex pathophysiology of NASH and suggested that some other companies developing therapies for NASH could benefit from Enanta’s research.
Enanta certainly isn’t the first company to fail to hit the mark in the NASH space. Nor is it the first company assessing an FXR agonist. Last year, Intercept Pharmaceuticals received a Complete Response Letter from the U.S. Food and Drug Administration for its experimental NASH treatment, obeticholic acid. Multiple companies have also struggled to achieve clinical success.
NGM Biopharmaceuticals failed to hit the mark in a Phase IIb study assessing aldafermin, an engineered analog of the human hormone FGF19, earlier this year, while GENFIT ended its development of elafibranor for NASH following a trial failure last year. There are more than 200 different treatments in development for NASH, but none of them have succeeded in the clinic so far.
NASH is a progressive liver disease caused by excessive fat accumulation in the liver, inducing chronic inflammation. That inflammation then results in progressive fibrosis, leading to cirrhosis, eventual liver failure, cancer, and death. Advanced fibrosis is associated with a substantially higher risk of liver-related morbidity and mortality in patients with NASH. The disease is projected to become the leading cause of liver transplants in the United States.
100 项与 TC-100 相关的药物交易
登录后查看更多信息
研发状态
10 条进展最快的记录, 后查看更多信息
登录
| 适应症 | 最高研发状态 | 国家/地区 | 公司 | 日期 |
|---|---|---|---|---|
| 胆汁淤积 | 临床前 | 意大利 | - | |
| 炎症性肠病 | 临床前 | 意大利 | - | |
| 非酒精性脂肪性肝炎 | 临床前 | 意大利 | - |
登录后查看更多信息
临床结果
临床结果
适应症
分期
评价
查看全部结果
| 研究 | 分期 | 人群特征 | 评价人数 | 分组 | 结果 | 评价 | 发布日期 |
|---|
No Data | |||||||
登录后查看更多信息
转化医学
使用我们的转化医学数据加速您的研究。
登录
或
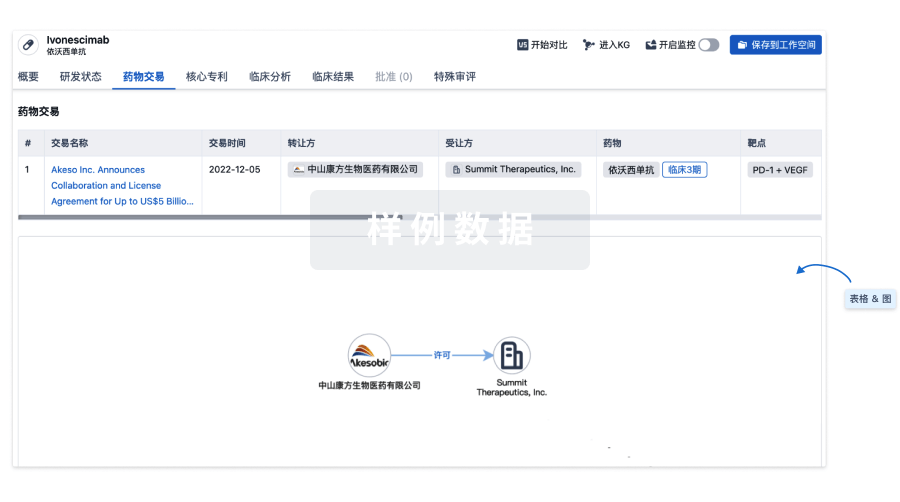
药物交易
使用我们的药物交易数据加速您的研究。
登录
或
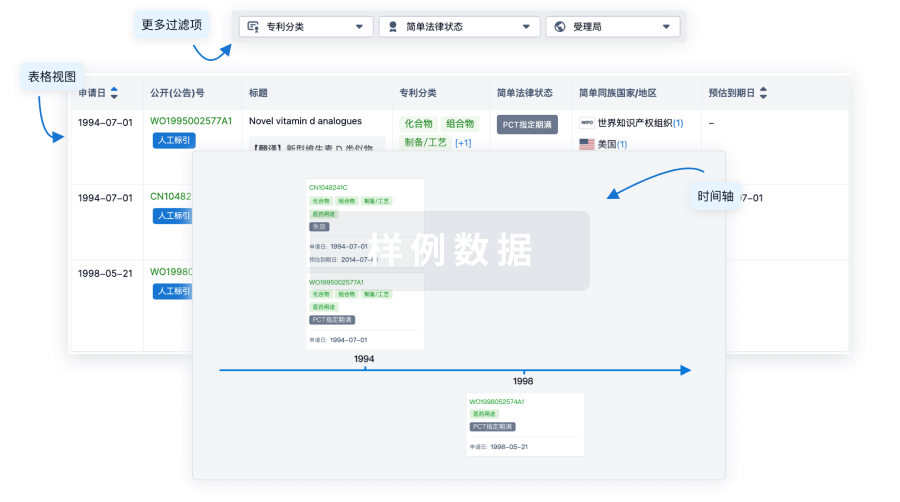
核心专利
使用我们的核心专利数据促进您的研究。
登录
或
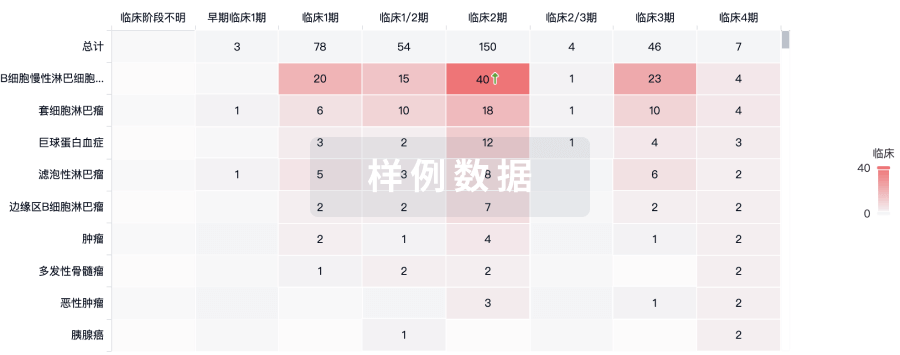
临床分析
紧跟全球注册中心的最新临床试验。
登录
或
批准
利用最新的监管批准信息加速您的研究。
登录
或

特殊审评
只需点击几下即可了解关键药物信息。
登录
或

来和芽仔聊天吧
立即开始免费试用!
智慧芽新药情报库是智慧芽专为生命科学人士构建的基于AI的创新药情报平台,助您全方位提升您的研发与决策效率。
立即开始数据试用!
智慧芽新药库数据也通过智慧芽数据服务平台,以API或者数据包形式对外开放,助您更加充分利用智慧芽新药情报信息。
生物序列数据库
生物药研发创新
免费使用
化学结构数据库
小分子化药研发创新
免费使用